")
Management of diabetic eye disease: an overview
Related content

Systemic risk factors
In order to reduce the risk of diabetic eye disease (both retinopathy and maculopathy) progressing and causing visual loss, it is important for all people with diabetes to maintain good overall health and good control over their diabetes. This is especially important for patients who already have diabetic retinopathy (DR) which is already affecting their vision, or is likely to damage it soon.
The two most important risk factors are high blood glucose (sugar) and high blood pressure.
High cholesterol and lipids also seem to be related to DR getting worse. Treatment of high cholesterol and lipids with statin medications, if available, reduces the risk of DR progressing. Maintenance of a healthy lifestyle overall will be beneficial for DR. This includes not smoking (or giving up) and getting regular exercise. People with diabetes should follow a healthy diet and avoid sugar and refined carbohydrates as much as possible.
Eye health professionals have a role in identifying patients at risk of sight loss from DR, and reinforcing messages about diabetes control and healthy living. Screening for DR and laser treatment for DR are both good opportunities for eye health professionals to get these messages across to patients.
Laser for DR and maculopathy
Laser is the mainstay of treatment for both DR and maculopathy. Table 1 summarises the indications, desired response indicators, insufficient response indicators and side effects of both, based on the articles below on preventing sight loss from DR and preventing sight loss from maculopathy. The glossary of terms below and the poster in the centre of this issue (pages 70–71) provide helpful background about the terms used.
Tips for successful laser
- Make sure that the patient has realistic expectations and is aware of the limitations.
- Ensure the laser focus and optical focus are together.
- Take care focusing the laser (aiming beam) and titrating the power.
- For pan-retinal laser, ensure that the temporal quadrant is adequately treated, up to the edge of the macula.
- For macular laser:
––cover the area of diabetic macular oedema (DMO) systematically, as laser uptake may be poor in the area of DMO
–– if the fovea is indistinct, laser outside the area which contains the fovea within it. - If attaining appropriate burn strength becomes difficult or variable, remove the contact lens and reapply coupling gel.
Table 1. Indications, response indicators and side effects of laser treatment for maculopathy and retinopathy
| Laser for diabetic retinopathy (DR): peripheral retinal photocoagulation (PRP) | Laser for maculopathy (focal or grid laser) | |
|---|---|---|
| Indications | Severe pre-proliferative DR 4-2-1 rule (see page 65) Proliferative DR Proliferative DR with high-risk characteristics (new vessels or vitreous haemorrhages) |
Clinical significant macular oedema (CSMO) Diabetic macular oedema (DMO) affecting the central fovea Exudates threatening/affecting vision |
| Desired response | Regression of new vessels Prevention of new vessel formation |
Reduction in DMO Prevention of (further) deterioration of vision |
| Insufficient response? | Reapply PRP, making burns more dense and extensive Keep repeating |
Once grid is complete over oedematous area (or macula in diffuse DMO) no benefit from further grid laser. Individual microaneurysms can be targeted. |
| Side effects and complications | Reduction in night vision and peripheral vision Initiating/worsening DMO Foveal burn (rare) |
Foveal burn Paracentral scotomas for deliberately close laser shots |
Glossary
Clinically significant macular oedema (CSMO)
CSMO is when leakage from small retinal blood vessels causes macular oedema (retinal swelling) and exudates (fat deposits from the blood) which are sufficiently close to the fovea (central macula) to affect or threaten the vision.
Diabetic maculopathy
Diabetic maculopathy is part of diabetic retinopathy. Maculopathy is damage to the macula, the part of the eye responsible for central vision.
Diabetic macular oedema (DMO)
Diabetic macular oedema occurs when blood vessels near to the macula leak fluid or protein onto the macula.
Diabetic retinopathy (DR)
Diabetic retinopathy occurs when changes in blood glucose levels cause changes in retinal blood vessels. In some cases the vessels leak fluid into the macula part of the retina which swells up (DMO). In other cases, abnormal blood vessels will grow on the surface of the retina.
Peripheral retinal photocoagulation (PRP)
Cauterisation of the peripheral retina using laser, with a minimum of 2,000 effective burns.
Proliferative diabetic retinopathy
This is the advanced stage of diabetic retinopathy. New blood vessels grow along the inside surface of the retina and into the vitreous gel, the fluid that fills the eye. These vessels are fragile and more likely to leak and bleed. Scar tissue is formed and can contract and cause retinal detachment (the pulling away of the retina from underlying tissue) – which results in blindness.
The Early Treatment in Diabetic Retinopathy Study (ETDRS)
The Early Treatment in Diabetic Retinopathy study (ETDRS) has produced over 20 publications. View the list on the ClinicalTrials.gov website.
ETDRS and the preceding Diabetic Retinopathy Study are summarised in Chapters 1 and 2 of Clinical Trials in Ophthalmology, Eds PJ Kertes and MD Conway. Lippincott Williams and Wilkins 1998.
Preventing sight loss from proliferative diabetic retinopathy
The keys to preventing sight loss from proliferative DR are as follows.
- Identify the right patients to treat with peripheral retinal photocoagulation (PRP). PRP is destruction of the peripheral retina using laser, with a minimum of 2,000 effective burns.
- In those with established new vessels, treat them with enough PRP and, if the response to PRP is insufficient, keep going with more and more.
When to do laser
In patients with obvious new vessels at the disc (NVD) or elsewhere in the fundus (NVE), or if there is some vitreous haemorrhage associated with new vessels, it is a straightforward decision: treat them with PRP. (These are called ‘high-risk characteristics’ because there is a high risk of visual loss in the ensuing years.)
There are also benefits to treating patients with less advanced DR. The Early Treatment in Diabetic Retinopathy Study (ETDRS) showed that PRP treatment can prevent these patients from progressing to the high-risk state. In a resource-poor setting where follow-up of patients may be haphazard, or patients are unable to attend for regular appointments, treating patients with less severe disease will prevent them getting worse. The threshold which ETDRS has established for laser has become known as the 4-2-1 rule (see panel below) and equates to severe pre-proliferative DR. Patients with this level of DR and above should be treated.
The 4-2-1 rule
The 4-2-1 rule is:
- 4 quadrants of the fundus with dense retinal haemorrhages and microaneurysms; or
- 2 quadrants with venous beading; or
- 1 quadrant with intra-retinal microvascular abnormalities (IRMA).
These are all signs of retinal ischaemia, which is the stimulus for eventual new vessels– leading to tractional retinal detachment, vitreous haemorrhage and visual loss.
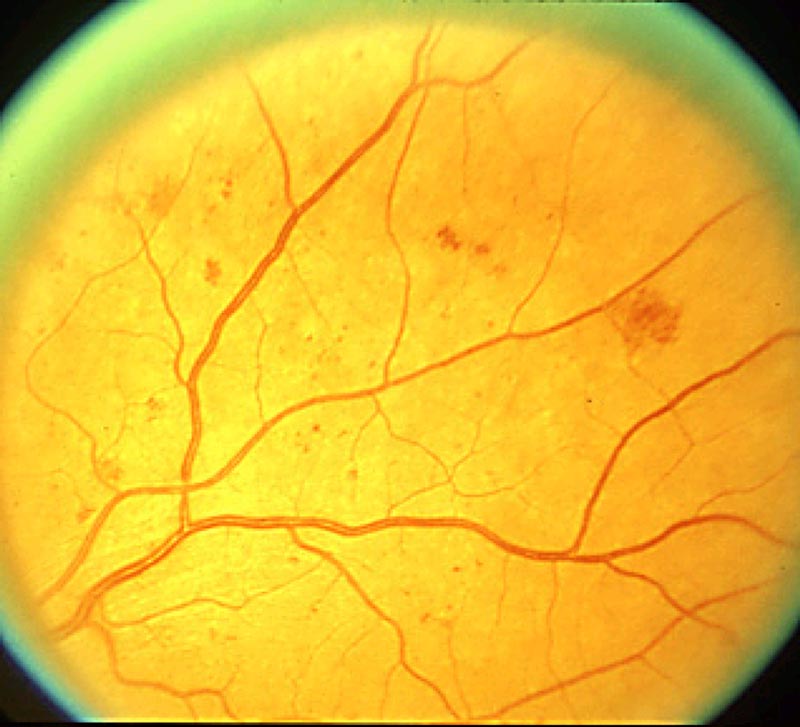
When are haemorrhages and micro-aneurysms dense?
The ETDRS study referred to standard photographs (Figure 1), if these are not available a rule of thumb is 5 or more haemorrhages and micro-aneurysms in a 1 mm wide slit, wherever in the quadrant you place the slit with a 90D lens.
Venous beading is clear dilation of retinal venules with accompanying constriction so it looks like a string of sausages.
IRMAs are abnormal branching, or network of vessels within the retina. ETDRS used standard photographs to define the size of IRMA that was significant. In a low- or middle-income country setting, with unreliable follow up, any definite IRMA warrants laser treatment.
Cotton wool spots are also a sign of retinal ischaemia and tend to occur in the border between well-perfused and poorly perfused retina. Although not part of the threshold, cotton wool spots are important in gaining an assessment of retinal ischaemia particularly in the absence of fluorescein angiography. They can push the clinician towards laser treatment.
Remember, these signs tend to occur together, so where there are cotton wool spots or dense haemorrhages or micro-aneurysms, look closely for IRMA or venous beading.
Tips for successful laser
It is important that, before you start, the patient knows what to expect and what the aims of treatment and potential side effects are. In particular, you should stress that the laser treatment is to prevent visual loss in the future and is not intended to improve vision. At the start of the treatment, titrate the strength of the laser burn and adjust the laser power to achieve a visible burn which is not too harsh or bright white.
Remember: doubling the duration or power doubles the fluence (laser energy delivered per square millimetre), whereas halving the diameter increases the fluence by a factor of 4.
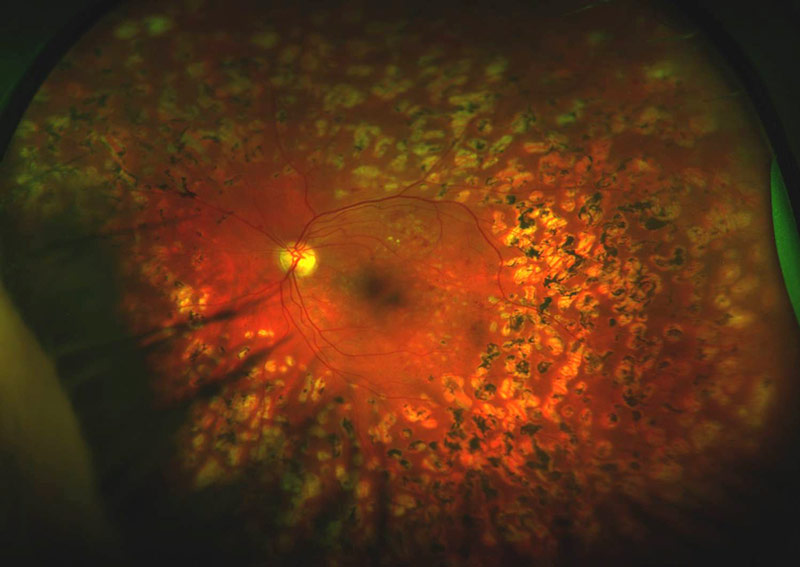
Modern spot sizes are smaller than in the ETDRS era, 200 microns being the standard. The duration of each laser burn is also shorter, and I recommend 0.02 s (20 ms). This reduces the laser injury and you do not have to worry about lasering over retinal vessels with this short duration. I start with 200 mW laser power if there is a clear lens. In patients with lens opacity, more power is required. Increase the power in 50 mW steps until a burn is visible. If it is too harsh (it will appear white, with a sharply defined edge), turn the power down in 25 mW steps (Figure 2). The central retina is thicker than the peripheral retina, so if you start centrally, you will have to reduce the power as you treat more peripheral retina.
The temporal quadrant is often undertreated and a zone of significant ischaemia, as it is a watershed between the vascular arcades. The laser should be brought up to the temporal edge of the macula, approximately 2 disc diameters from the foveal centre. It helps to define this border temporally with laser burns and work progressively peripherally away from it to avoid inadvertent macular coverage, or worse, a foveal burn. The clinician should know where the macula is at all times.
NOTE: If during the treatment you have lost visible burns with the fluence unchanged, it is usually either a focusing issue or loss of coupling gel in the contact lens. Pause, detach the lens, refill with gel and continue.
To treat pre-proliferative disease, 2,000 to 3,000 effective burns are usually sufficient, particularly if you are relatively certain that the patient will return for an examination and further treatment if needed. With proliferative DR, more burns may be required.
Call patients back for a follow-up visit to see if the new vessels regress over the following 3–6 months. If they are not regressing, more treatment is needed. In this scenario, you should treat between the original burns, up to 500 microns from the nasal disc edge and within the arcades, with two or three burn rows and as far into the peripheral retina as you can reach with your lens. Around 5,000 burns may be required.
White fibroglial tissue will not disappear, but you are aiming to get the vascular component to regress. However, the longer the new vessels have been present (often associated with glial tissue), the harder it will be to get them to regress completely. It is okay to accept incomplete regression if the situation is stable, and you have done as many burns as you think is reasonable.
If there is vitreous haemorrhage it is very important to apply as much laser treatment as possible, as quickly as possible, whilst there is a view. There may be a small vitreous haemorrhage with scope for laser, before a larger one obscuring your view prevents any treatment. Where there is a small vitreous haemorrhage, laser is therefore urgent – because any subsequent and more severe haemorrhage is likely to have a much better outcome if the DR had been treated before the haemorrhage occurs.
Complications and side effects of peripheral retinal laser (PRP)
PRP inevitably sacrifices some peripheral retina, but in most cases this does not have any effect on vision. In about 10% of cases, patients notice a reduction in visual field or night vision.
The effect on night vision may be more noticeable in low-income countries, where night vision is essential. The more PRP is required, the more likely this is to be an issue and it may affect the person’s ability to drive. This is a trade-off with preserving any vision at all.
A foveal burn, affecting central vision, is possible but should not happen if the operator makes sure where the macula is at all times, and only switches the equipment from ‘standby’ to ‘treat’ when she or he is ready to start lasering.
Macular oedema can be induced by an aggressive and extensive PRP session. This can damage the patient’s confidence by making the vision worse afterwards. If possible PRP should be offered in two treatment sessions of about 1,500 burns each to avoid this. If necessary, macular laser should be applied before PRP, or at least at the same time as the first session if the PRP is urgent.
Role of antiVEGF in PDR
Intra-vitreal anti-VEGF injections such as bevacizumab (Avastin) only buy time until more definitive treatment. One special situation in which they might be of benefit is where severe ischaemia has led to rubeotic glaucoma. An injection of bevacizumab can induce regression of new vessels, reduce IOP, improve pupil dilation and allow laser application. Bevacizumab can be used just prior to vitrectomy to reduce bleeding during surgery and make it technically easier. However, new vessels may recur aggressively if definitive laser treatment is not commenced within a month.
Surgery for proliferative DR
Vitrectomy surgery has limited availability, particularly in sub-Saharan Africa. Early treatment with laser should reduce the need for vitrectomy, however patients will inevitably present late particularly with vitreous haemorrhage resulting in sudden visual loss. This is the commonest indication for vitrectomy in DR. Where there is any view of the fundus, PRP is indicated. When there is not there are two scenarios: the patient who has had previous PRP and the patient who has not. If a patient has previously had a complete PRP then you can afford to wait and the haemorrhage will usually clear. There may be traction on a non-regressed new vessel but active neovascularisation should not be progressing. Where a patient has had no previous PRP the disease is actively progressing behind the haemorrhage. Here an early vitrectomy is indicated if available, usually with pre-treatment by an injection of anti-VEGF. If vitrectomy is impossible, then you can monitor and apply laser to visible zones as soon as there is any clearing.
The other indication for vitrectomy in PDR is progressive tractional retinal detachment (TRD) affecting the macula. TRD elsewhere does not require surgery. Unfortunately the eventual outcome is often poor because of the accumulated damage to retinal function, including ischaemic maculopathy.
Preventing sight loss from maculopathy
Laser treatment is less successful at reducing the risk of diabetic macular oedema (DMO) causing visual loss compared to peripheral retinal photocoagulation for proliferative diabetic retinopathy. Intravitreal treatments are effective but often unavailable due to cost and access to treatment.
When to do macular laser
The threshold for macular laser is usually clinically significant macular oedema (CSMO) as defined in the Early Treatment of Diabetic Retinopathy Study (ETDRS). CSMO is any retinal thickening (oedema) and/or exudates within 500 microns (⅓ disc diameter) of the centre of the fovea; or oedema greater than 1 disc area within 1 disc diameter of the foveal centre – including oedema which involves the fovea already. Macular laser is more effective if the DMO is localised (focal maculopathy), than if it is generalised across the central macula (diffuse maculopathy). Optical Coherence Tomography (OCT) scans enable visualisation of macular oedema in great detail, but are not required to determine whether a patient meets the thresholds for macular laser, because these were determined prior to the advent of OCT.
Exudates, if they involve the fovea, can sometimes threaten or affect vision without macular oedema. Exudates without oedema within 500 microns of the foveal centre, particularly long or streak exudates pointing towards the centre, are an indication for laser.
Tips for successful macular laser
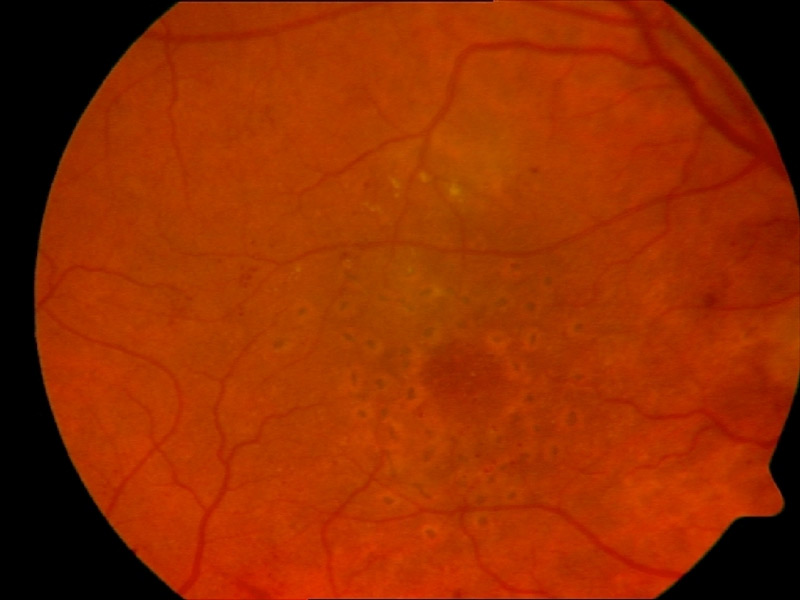
Macular laser is much more gentle and measured than peripheral retinal photocoagulation (PRP). Macular laser can be directed at microaneurysms, or applied in a grid pattern over the oedematous zone. Macular laser is usually given as a combination of both, which is known as a Modified Macular Grid: the microaneurysms are targeted first, and untreated areas of oedema are then treated in a grid pattern (see Figure 3).
Although it is important to make sure that the laser beam is focused in PRP, this is critical in macular laser. Retinal lasers are not in a parallel beam but converge to a focus. Whilst setting up the laser, make sure that the laser focus and the optical focus of the slit lamp are in the same plane. Lasers are usually supplied with a test rod, but the focus adjustment can be done on the fundus with the laser in standby. Focus the aiming beam, and then adjust each eyepiece until the view is also in focus.
For macular laser:
- The default laser spot size is 100 microns; however, smaller sizes can be used if small microaneurysms are being targeted and the patient is very still.
- Short durations, such as 0.02 s, result in less retinal damage but may need to be increased for microaneurysm treatment.
- The power should be low to start with (100 mW) and increased in steps of 50 mW as necessary (the same as for PRP). However, the desired burn should be just visible (less visible than for PRP).
- Titrate the laser power away from the fovea, on the edge of the macular oedema. This is because uptake is less good within zones of oedema. It may be necessary to increase the power in zones of oedema, but limit this to an increase of 100mW.
- For a first macular laser treatment, the laser burns should be 750 microns (half a disc diameter) from the centre of the fovea. If the fovea is hard to discern then the inner ring should be wider, outside the zone including the fovea.
- Most operators like to start with the inner ring after titrating the laser power, and then move outwards to complete 4–6 rings. This should create an adequate grid to treat a diffuse maculopathy.
- If further treatment is required, and the patient can keep still, a further ring, 500 microns (⅓ disk diameter) from the centre, can be added. However, once the grid is complete there is nothing to be gained by further grid laser. This is unlike PRP, where fill-in laser can be repeated many times if necessary.
- When targeting microaneurysms, the ideal result from laser is a colour change. However, it is difficult to land a direct hit with one shot, and not more than 5 attempts should be made on an individual microaneurysm. As microaneurysms occur in the thickened retina, it may be necessary to focus slightly anteriorly to treat them accurately.
- The spaces between burns for the grid laser should be approximately the width of 1 spot.
Macular laser takes 8 weeks to a year to have its full effect so do not rush to judge it. The main aim is to prevent deterioration of vision, and the recent trials with a laser cohort show that stable vision is about what is achieved on average. However, for focal maculopathy with good vision, maintenance of that good vision with laser is well worthwhile.
Complications of macular laser
The complication to be avoided in macular laser is foveal burn. This can occur if:
- Microaneurysms closer than 500 microns (⅓ disc diameter) from the foveal centre are targeted.
- If care is not taken to avoid the whole central macula when the position of the fovea is unclear.
- If the patient moves suddenly.
The worst scenario is immediate loss of central vision, but with short laser durations this can be mitigated. Sometimes patients are aware of paracentral scotomas from the laser burns if they are close to the foveal centre – it is therefore important to listen to what they have to say.
Role of intravitreal treatment in maculopathy
Recent studies have shown that anti-VEGF treatment produces greater visual improvements than laser in patients with central diabetic macular oedema (DMO) whose vision is reduced to 6/12 or worse. These intravitreal injections reduce DMO rapidly and effectively. Laser treatment usually prevents loss of vision but does not often lead to visual improvement. Repeated injections of bevacizumab in eyes with visual acuity of less than 6/12 give an average improvement of two lines on the Snellen chart, and about a quarter of patients will improve by three lines. However, they have a number of problems – notably cost, the treatment burden of monthly injections, and the risk of infection/endophthalmitis. Even the relatively low cost of bevacizumab is prohibitive to many patients in low- and middle-income countries. Furthermore, a reliable pharmacy is required, one which can divide the intravenous dose into intravitreal doses in sterile conditions. Clusters of endophthalmitis cases in the US and UK have led to a suspicion of contaminated batches of anti-VEGF preparations. This is a definite concern in less well-regulated areas.
Evidence from clinical trials suggests that patients require 9–12 injections in the first year, so the treatment regime is intense – requiring frequent revisits in order to maximise the benefits. After the first year, the overall treatment burden is less, but some patients have recurring DMO requiring ongoing retreatments. Despite these problems, the greater effectiveness of intravitreal injections means that they may be valuable for some patients, particularly those who can afford the drug costs and live sufficiently near to the clinic to attend for repeated treatment.
An alternative intravitreal treatment is steroid, the least costly being triamcinolone. This is effective, but visual gains are reduced by induced cataract, and even after cataract surgery on average the vision does not catch up with that from anti-VEGF therapy. This may be due to exacerbated DMO or postoperative cystoid macular oedema. Intravitreal steroid is an option, especially in patients who are already pseudophakic. Post-injection intraocular pressure (IOP) rise can be a problem, so this needs to be monitored and treated accordingly.