")
Neonates at risk of retinopathy of prematurity in Paraguay
Related content
Retinopathy of prematurity (ROP) is a vasoproliferative retinopathy which can occur in premature babies as a result of interruption of the normal process of retinal vascularisation. The earliest signs usually occur 5-7 weeks after birth, and are characterised by a demarcation line at the junction of the vascularised and avascular peripheral retina (Stage 1). Subsequently a distinct ridge forms (Stage 2), followed by extraretinal fibrovascular proliferation (Stage 3). ‘Plus’ disease exists when there is arterial tortuosity and venous dilatation in the posterior segment, and breakdown of the blood ocular barriers. Sub-total and total retinal detachment (Stage 4 and Stage 5) may develop. The extent of retinopathy is described in terms of clock hours, each clock hour representing a 30° segment of a 360° circle. Although spontaneous regression is common in Stages 1, 2 and early Stage 3 disease, careful observation is required to detect babies who progress to stages of ROP that need treatment, i.e., the presence of ‘threshold disease’, defined as Stage 3 ‘plus’ disease with 8 or more total clock hours of involvement, or 5 or more continuous clock hours of involvement. Treatment should be by laser or cryotherapy to the avascular peripheral retina, which prevents progression to Stages 4 and 5 in approximately 50% of cases.
Childhood visual loss due to ROP was very rare prior to 1944. This changed dramatically with the administration of supplemental oxygen to preterm infants in the late 1940s. By 1950, ROP was the commonest cause of blindness in children in western countries. With the implication of hyperoxia in the pathogenesis of ROP, oxygen restriction decreased the incidence of blindness from ROP in the mid 1950s to mid 1960s.
Advances in neonatal intensive care since the 1960s have increased the survival of low birth weight (LEW; less than 1,500 gms) and extra low birth weight babies (ELBW; less than 1,000 gms), and in the west ROP now occurs mainly in ELBW babies. Low birth weight and preterm birth are considered the most important factors to determine infants at risk of ROP. Other factors that are associated with ROP include apnoea and respiratory distress.
Data from blind school studies carried out in Chile1 and Paraguay2 in 1992 show that ROP was responsible for 18% of childhood visual loss in both countries. In 1994 the proportion of blindness in children in schools for the blind in Paraguay had increased to 33%.3 Before planning a nation-wide screening programme for the detection and treatment of ROP, there is a need to determine how many babies are at risk of ROP. For Latin America, the degree of risk based on birth weight is probably as follows:4
- Birth weight >1750 grams: Very low risk
- Birth weight 1501-1750 grams: Low risk
- Birth weight 1250-1500 grams: Moderate risk
- Birth weight 1000-1249 grams: High risk
- Birth weight <1000 grams: Very high risk
Table 1. Number of live births in Paraguay weighing < 1500 grams from May 1993 – April 1994, and survival rates in the different neonatology
| Public hospitals | Born alive | Survived | Outcome unknown | %survival* (95% CI) |
|---|---|---|---|---|
| Hospital de Clinicas, Asuncion | 52 | 18 | 0 | 34.6 |
| Hospital I.P.S., Asuncion | 50 | 14 | 1 | 28.6 |
| Gran Hospital Nacional, Itagua | 49 | 33 | 1 | 68.8 |
| Hospital Cruz Roja, Asuncion | 49 | 16 | 0 | 32.7 |
| Hospital Regional, Ciudad del Este | 35 | 4 | 2 | 12.1 |
| Hospital Regional, Encarnacion | 20 | 7 | 3 | 41.2 |
| Hospital Pediatrico Municipal, Encarnacion | 6 | 3 | 1 | 60 |
| Subtotal | 261 | 95 | 8 | 37.5 |
| (31.5-43.5) | ||||
| Private hospitals: | Born alive | Survived | Outcome unknown | %survival* (95% CI) |
| Centro Medico Bautista, Asuncion | 7 | 4 | 0 | 57.1 |
| Hospital Migone Battilana, Asuncion | 6 | 5 | 0 | 83.3 |
| Hospital de Itaipu, Ciudad del Este | 6 | 5 | 0 | 83.3 |
| Hospital Italiano, Asuncion | 5 | 1 | 2 | 33.3 |
| Hospital Filadelfia, Fernheim | 2 | 1 | 0 | 50 |
| Hospital Adventista, Asuncion | 1 | 1 | 0 | 100 |
| Hospital Privado del Nino, Asuncion | 1 | 1 | 0 | 100 |
| Sanatorio Manuel Riveros, Ciudad del Este | 1 | 1 | 0 | 100 |
| Subtotal | 29 | 19 | 2 | 70.4 |
| (53.2-87.6) | ||||
| Total | 290 | 114 | 10 | 40.7 |
* excludes babies who were transferred and where the outcome was not known
95% CI = 95% confidence interval
This retrospective study was undertaken to determine the number of babies at risk of ROP born in Paraguay during a one year period.
Method
Data were collected on all live-born infants weighing less than or equal to 1,500 grams at birth born between 1 May 1993 and 30 April 1994 from all the hospitals in Paraguay with neonatology units (private and public). On examining the records of many other hospitals in Paraguay, it was clear that of the estimated 29,000 live-born infants in Paraguay per year, those weighing less than 1,500 grams do not survive outside neonatal units. The upper limit of 1,500 gms was chosen due to the low risk of ROP in infants larger than 1,500 grams at birth. In addition to birth weight, data were collected on name (for reference purposes), birth date, gestational age, sex, and date of death or discharge from the hospital.
Results
A total of 290 live births weighing less than or equal to 1,500 grams were recorded. Records of 10 infants transferred to other hospitals for further neonatal care were not found in the other hospitals, and as their outcome was not known they have been excluded from the survival data. Of those with complete data (280), 114 survived to leave hospital giving an overall survival rate of 40.7% (Table 1). The survival rate in seven public hospitals was 37.5% compared with 70.4% in eight private hospitals. In the 6 units with 20 or more live-born low birth weight babies the survival rates varied widely, from 12% to 69%.
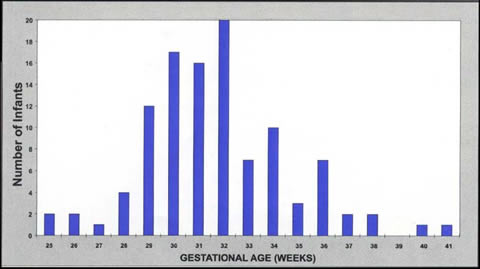
The birth weights of infants that left hospital alive ranged from 720 to 1,500 grams (mean 1,270 grams). There were 10 babies (9%) in the very high risk group (< 1,000 grams at birth), 34 babies (30%) at high risk (1,000-1,249 grams) and 70 (61%) at moderate risk of ROP (1,250-1,500 grams) (Table 2). The gestational ages of these surviving babies ranged from 25 to 41 weeks with a mean of 32 weeks, although 7 infants’ gestational ages were not recorded and have been excluded (Fig. 1). Fifty-four of the 114 surviving babies (47%) were born at less than 32 weeks gestation, and 61% were female.
Discussion
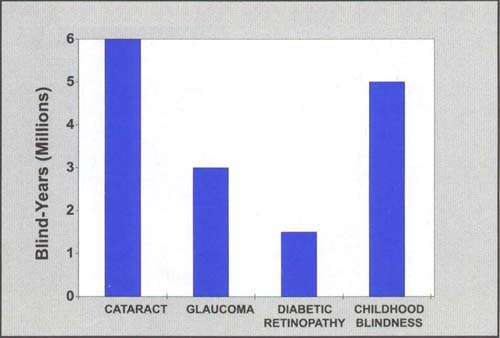
Childhood blindness is a world-wide problem with huge social and economic implications. It is estimated that 100,000 children are blind in Latin America.3 When considered in terms of blind years (i.e., number of individuals blind x estimated life expectancy), childhood blindness is almost equal in magnitude to blindness due to adult cataract (Fig 2). There is evidence that ROP is becoming a significant cause of blindness in children in some Latin American countries, and, as a potentially avoidable cause, requires urgent attention.
This study has shown that the overall survival rate of low birth weight babies born in Paraguay between May 1st, 1993 and April 30, 1994 was 40.7%, and that there were 114 surviving low birth weight babies. Differences exist between the survival rates of neonates cared for in the different units, but the number of babies cared for varies widely, making statistical comparison unreliable. Overall survival of low birth weight babies in the private sector was higher than in babies cared for in the government sector. This may be due to differences in the level of neonatal intensive care provided, or may reflect referral patterns.
In Europe and the USA, the mean birth weight of infants developing Stage 3 ‘plus’ disease or worse is 800-850 grams. This is a much lower value than the average of 1,050 grams encountered in children blind due to ROP in schools for the blind in Chile (Gilbert, personal communication). A lower quality of neonatal care may therefore increase a low birth weight infant’s risk of ROP. This implies that the infants born at the centres with lower neonatal survival rates in Paraguay may be more at risk of ROP than their counterparts in the better equipped units.
During the one year period of this study 114 low birth weight babies survived to leave hospital, and of these nearly half were born at less than 32 weeks gestational age. Consequently, there is a considerable number of infants with moderate to very high risk of ROP. A recent study of the same risk group for ROP in Argentina showed that of 244 infants examined, 7.3% developed threshold disease or worse.6 If considered valid for Paraguay, this would imply that approximately 8 infants go blind in Paraguay due to ROP on an annual basis, resulting in approximately 400 blind years annually.
Table 2. Survival rates of low birth weight babies in Paraguay by birth weight
| Level of risk of ROP | Very high | Very high | Very high | Very high | Very high | High | Moderate | Total |
|---|---|---|---|---|---|---|---|---|
| Birth weight | 500-599 | 600-699 | 700-799 | 800-899 | 900-999 | 1000-1249 | 1250-1500 | |
| Number of live births | 7 | 9 | 16 | 18 | 27 | 86 | 127 | 290 |
| Outcome not known | 0 | 0 | 0 | 0 | 0 | 4 | 6 | 10 |
| Number survived | 0 | 0 | 1 | 1 | 8 | 34 | 70 | 114 |
| (%) | (0%) | (0%) | (6.3%) | (5.6%) | (29.6%) | (41.5%) | (57.9%) | (40.7%) |
The blind school data from Paraguay seem to suggest that blindness due to ROP may be increasing. As a potentially preventable cause of childhood blindness, the treatment of ROP in Paraguay would therefore result in a significant reduction in the total number of blind years. Of the institutions visited, only the Gran Hospital Nacional in Itagua reported regular screening of low birth weight infants for ROP. Health care workers at other neonatology centres were generally unaware of the problem of ROP. Although carrying out the research for this study has already promoted some awareness of ROP among personnel at the hospitals visited, it is clear that much work needs to be done in order to establish regular communication between neonatologists and ophthalmologists. Neonatologists should be encouraged to arrange for examinations of all infants at risk of ROP, although without further research it is not clear exactly which babies should be included in screening programmes in Latin American countries.
The criteria for screening in European countries, the United States and Canada (i.e., those weighing less than 1,500 gms at birth, and/or born at less than 32 weeks gestation)7 may not include all babies at risk of ROP in Latin America. The criteria should probably be extended to include babies with birth weights of less than 1,750 gms, although this will increase the workload considerably. Examination of babies should be undertaken using an indirect ophthalmoscope and 20D or 28D lens. Care should be taken to examine the retinal periphery, using gentle scleral depression if necessary. The first examination should take place 6-7 weeks after birth irrespective of birth weight or gestational age, and examinations should be repeated every 2 weeks until one of the following has occurred:
- the retinal periphery has vascularised;
- stage 1, stage 2 or stage 3 disease shows definite signs of regression or
- stage 3 threshold disease has developed.
If the latter occurs, treatment should be given as a matter of urgency, as retinal detachment is likely to occur in 50% of eyes within the next 1-2 weeks.
Ultimately, a nation-wide screening programme should be organised in Paraguay, such that services can be provided in public as well as private hospitals. This could be accomplished by selecting one ophthalmologist with particular interest and adequate training in paediatric ophthalmology to carry out all examinations of infants at risk for ROP in Paraguay. The results of such a programme would be likely to cause significant reduction in the incidence of ROP, as well as childhood blindness as a whole in Paraguay.
Acknowledgments
Special thanks to Dr Clare Gilbert for her suggestions and advice, as well as to Hans-Heinrich Duerksen, Fabio Sabourgnan and Doris Loewen for their part in collecting the data. In addition, thank you to The University of Manitoba, The Canadian Society for International Health and The Canadian International Development Agency for their support in this endeavour.
References
1. Gilbert C, Canovas R, Kocksch, Foster A. Causes of blindness and severe impairment in children in Chile. Dev Med Child Neurol 1994;36: 326-33.
2. Duerksen R. Unpublished data. Presented at the workshop on childhood blindness held in Concepcion, Chile, November 1992.
3. Duerksen R. Unpublished data.
4. Prevention of Childhood Blindness. Proceedings of the workshop held in Concepcion, Chile, November 1992.
5. Foster A. Childhood Blindness in Latin America. Proceedings of the workshop held in Antigua, Guatemala, July 1992.
6. Iribarren G, Badier JA, Dilascio D, Zabalo E. ROP: Incidencia y tratemiento. Presented at the annual meeting of the Argentinian Society of Ophthalmology held in Buenos Aires, Argentina, July 1994.
7. Levene M, Garner A, Johnston S, Rennie J, Schulenburg E, Fielder A. Screening for retinopathy of prematurity. Working Party Report, College of Ophthalmologists, London. 1990.