")
Advances in the understanding of primary angle-closure as a cause of glaucomatous optic neuropathy
Related content
In the last few years the classification of angle-closure glaucoma has undergone revision. This is a result of population research in regions where angle-closure glaucoma is a major cause of blindness. Several studies have shown that most cases of angle-closure that cause glaucomatous optic neuropathy occur without the symptoms that Western ophthalmologists associate with episodes of acute angle-closure.1-3 We have, therefore, started using the classification scheme detailed in Table 1 in our research.
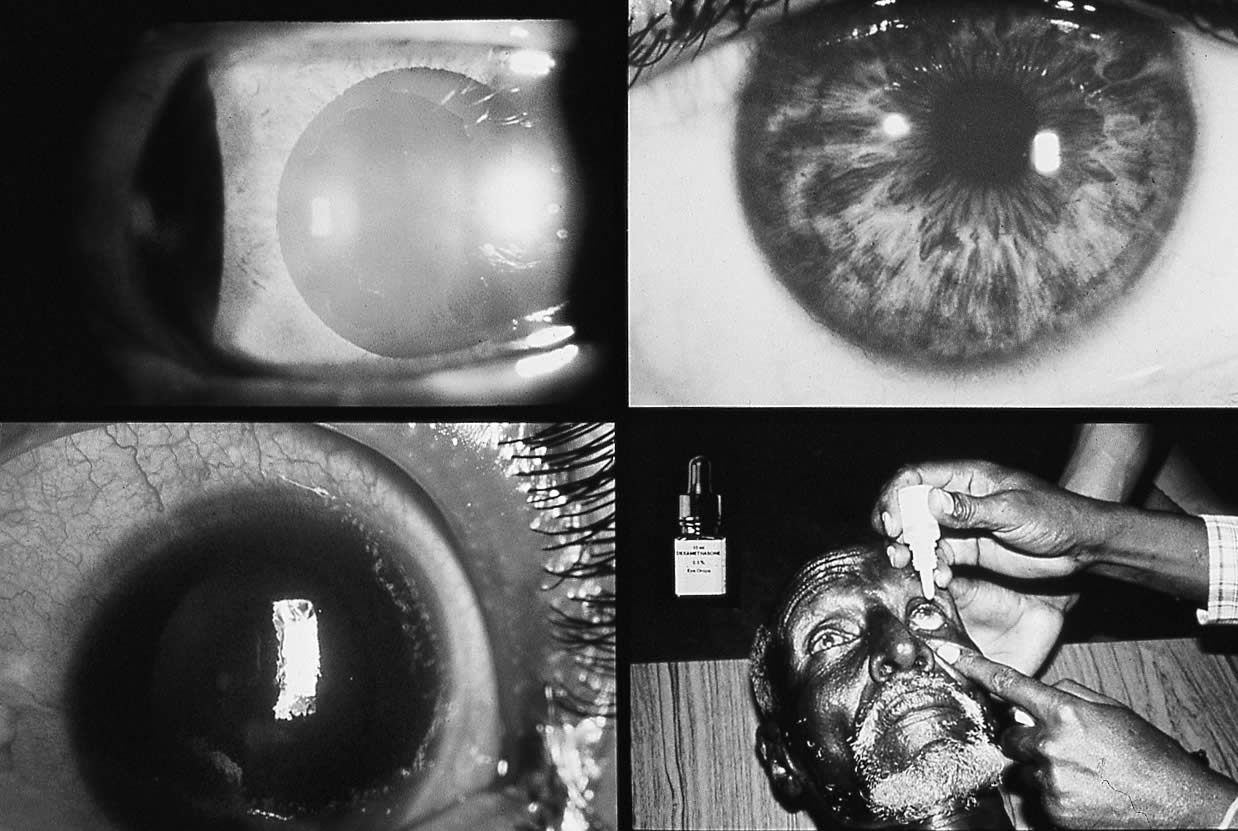
Other ocular tissues may be damaged by angle-closure. These are illustrated in Fig. 1. Damage to different structures should be specifically described when recording case details.
Prevalence of angle-closure
Ethnicity
Ethnic background is one of the major factors determining susceptibility to primary angle-closure (PAC). Population surveys show PAC is more common among people of Asian descent than those from Europe. Among people aged 40 years and over, the prevalence of PAC (the number of cases present at one point in time) ranges from 0.1% in Europeans,4 through 1.4% in East Asians 2,5 and up to 5% in Greenland Inuit.6 In Africa, a clinic-based study found the rate of primary angle-closure (gonioscopically verified closure of the angle with raised IOP) was equal among the black and white populations of Johannesburg. Among the white population 66% of cases were symptomatic, whereas only 31.5% of the black patients reported symptoms.7
Age and gender
The manifestations of ocular damage resulting from primary closure of the drainage angle are rare before the age of 40 years. After this, the prevalence of disease increases with age.1,2 Female gender is recognised as a major predisposing factor toward development of PAC. The prevalence of occludable drainage angles, PAC and PACG (Table 1), all tend to be higher in women than men. 1,2
Incidence of angle-closure
While prevalence is the standard measure of population morbidity at a specific time, events that are of short duration are more effectively quantified by calculating incidence (the number of new cases occurring over a specified period). The acute, symptomatic form of PAC is one such event. Incidence figures (given as cases/100,000 persons/year for the population aged 30 years and over) range from 4.7 in Finland to 15.5 in Singapore. As with prevalence, incidence increases with advancing age and shows that an excess of females are afflicted.8


Ocular characteristics associated with angle-closure
A shallow anterior chamber has long been recognised as a factor that predisposes toward angle-closure. The depth of the anterior chamber reduces with age and tends to be shallower in women than men.9 Ethnic groups that have a high prevalence of PAC have shallower anterior chambers.9
The depth of the anterior chamber is determined by the position of the lens within the globe, which in turn determines the width of the drainage angle. Although the relationship is not a simple geometric one, we examined anterior chamber depth (using an optical pachymeter) and gonioscopic configuration (assessed in four quadrants, using Shaffer’s grading scheme) in 942 Mongolians, aged 40-87. We found that 74% of variation in the width of the drainage angle could be explained solely on the basis of variation in anterior chamber depth (Foster PJ, Baasanhu J, Johnson G J: 1995 Unpublished).
Refractive status, anterior chamber depth, lens thickness and axial length are usually associated. Anterior chambers are shallower in hypermetropes than in myopes. Angle-closure is typically associated with a hypermetropic refractive state. Increasing living standards and higher educational attainment in Asian and Inuit populations seem to have been paralleled by an increasing prevalence of myopia.10,11 In Singapore, half the male Chinese population aged 15 to 25 years is myopic. Among those with a university education, this figure rises to 66%.10 This raises the question of whether the high rate of PAC previously encountered in these populations is destined to decline.
Screening for primary angle-closure glaucoma: an international perspective
Glaucoma is now probably the leading cause of irreversible blindness world-wide. It is suggested that 73 million people suffer from glaucoma, and, in 1996, Quigley estimated that 6.7 million were blind.12 The population of Asia account for the majority of this number and in a recent study of the prevalence of glaucoma in Singapore, we found that only 24% of POAG sufferers were blind in at least one eye, but 57% of PACG sufferers were blind in one eye. This difference was highly significant. 3
The epidemiology and natural history of POAG are relatively well understood. Until recently the epidemiology of PACG was not as clearly understood, but over the last 5 years there has been an increased research effort, and this deficiency is gradually being re-dressed. Previously, IOP was held to be the most suitable risk-factor for POAG that could be used for screening. However, although raised IOP is sufficient to cause glaucoma, it is not necessary. Between one-half and two-thirds of POAG cases have an IOP consistently within the ‘statistically normal’ range. ~sychophysical tests and disc imaging techniques offer promise although the technology is immature and remains to be proven.
Anterior chamber depth
In contrast, PACG does have features that are more readily identifiable. Closure of the drainage angle requires the iris and the trabecular meshwork to be in relatively close proximity prior to the development of the closure process. The association between PACG and a shallow anterior chamber has prompted the investigation of measurement of central and limbal anterior chamber depth measurement as tools for screening for PACG.
In the context of a screening programme for PACG, the intention would be to detect persons with appositional angle-closure, in the ‘latent’ phase of the disease before glaucomatous optic neuropathy has developed. These people can be reliably detected by either measurement of the axial ACD (either by optical pachymetry or A-mode ultrasound), or grading of the limbal chamber depth by the van Herick technique where the slit-lamp beam is shone at right angles to the cornea at its periphery, close to the limbus. Both these tests will give a sensitivity and specificity of over 80%. Assuming a population prevalence of 5% for people aged 40 years and over with occludable drainage angles, this translates to positive and negative predictive values of the tests of 17% and 99%. These figures mean that 17% of people ‘failing’ the screening test and being referred for confirmatory examination will have occludable drainage angles. Put another way, about 1 out of 5 people referred to an ophthalmologist for gonioscopic examination would require treatment. One person in 100 would be incorrectly classified as normal.13,14
The suitability of the tests for mass screening varies. Both axial and limbal chamber depth grading have been used in the field on over 1,700 people in Mongolia, and were found to be acceptable and safe. The limbal chamber depth (van Herick) grading requires a slit-lamp, and probably an ophthalmologist or experienced technician. It is, therefore, limited by the need for sophisticated equipment and highly trained staff. Axial chamber depth measurement by optical pachymetry has the same limitations. Ultrasound measurement of anterior chamber depth with a hand-held probe avoids the need for a slit-lamp, but gives much less reproducible measurements than slit-lamp-mounted ultrasound.15 Using a hand-held device in a population-based screening programme would result in a small but significant degradation in test performance.13 Therefore, the ideal method would use a joy-stick directed ultrasound probe mounted on a stabilised base-plate with a chin-rest. It is envisaged that a self-contained screening kit would fit into a small suitcase. A prototype of this device is currently in production.
Table 1: Classification of Primary Angle-Closure
1. Primary angle-closure suspect
An eye in which appositional contact between the peripheral iris and posterior trabecular meshwork is considered possible.
2. Primary angle-closure (PAC)
(a) Non-ischaemic: an eye with an occludable drainage angle and features suggesting trabecular dysfunction, such as peripheral anterior synechiae, elevated intraocular pressure or excessive pigment deposition on the trabecular surface. The optic disc and visual field are normal.
(b) Ischaemic: the presence of iris whorling, stromal atrophy or glaukomflecken signify previous ‘acute’ PAC. However as these are areas of ischaemic necrosis,we suggest that ‘ischaemic PAC’ is the correct description. Differentiating between ischaemic and non-ischaemic PAC is supported by experimental evidence that the iris and ciliary body are the ocular tissues most sensitive to pressure-induced ischaemia. Damage to the optic nerve only occurs at higher pressures, and therefore anterior segment ischaemic sequelae indicate that nerve ischaemia may have occurred, but do not confirm it.
3. Primary angle-closure glaucoma (PACG)
Glaucomatous optic atrophy, with a characteristic visual field defect in the presence of an occludable drainage angle or signs of PAC.
Management
The next consideration, after detection, is the management of persons found to have occludable drainage angles. Prophylactic laser peripheral iridotomy (PI) offers a non-invasive, quick procedure that has few significant short-term complications. Probably the most significant complication from the point of view of care of a patient with glaucoma is the post-laser pressure spike, although adequate pre-medication should prevent this. However, pre-medication, either with topical apraclonidine or oral acetazolamide, may have serious side-effects. Use of apraclonidine has been associated with collapse in one elderly female patient undergoing laser treatment. The risk of erythema multiforme with acetazolamide is small but present. In a regional or national blindness prevention campaign where the number of people treated might run into thousands, these rare but severe adverse effects may become significant factors in the risk benefit equation.
More importantly, the efficacy of laser PI as a prophylactic measure for PACG is uncertain. It has been suggested that PACG in Asian people may often be caused by a non-pupil block mechanism, which would not be amenable to laser iridotomy. However, a follow-up study performed in 1998 looking at Mongolian people with occludable drainage angles treated in our 1995 and 1997 surveys found that the median angle width had increased by 2 Shaffer grades following laser PI. Patent peripheral iridotomies were found in 98%. Iridotomy alone failed in 3% of eyes with narrow drainage angles and either peripheral anterior synechiae or raised IOP, but normal optic discs and visual fields. However, in eyes with established glaucomatous optic neuropathy at diagnosis, iridotomy failed in 47%. None of the eyes with narrow angles that were normal in all other respects and underwent iridotomy, developed glaucomatous optic neuropathy or symptomatic angle-closure within the short follow-up period. This suggests that Nd:YAG laser iridotomy is effective in widening the drainage angle, and reducing elevated IOP in East Asian people with primary angle-closure without glaucomatous optic neuropathy.
Furthermore, it suggests that pupil-block is a significant mechanism causing closure of the angle in this population. Once glaucomatous optic neuropathy associated with synechial angle-closure has occurred, iridotomy alone is less effective at controlling IOP 16 and trabeculectomy will usually be necessary.
Conclusion
The understanding of the epidemiology and management of primary angle-closure has advanced considerably in the last decade. PACG is possibly the leading cause of blindness in East Asian countries. There is great interest in the natural history of narrow drainage angles and eyes with PAC. Only longitudinal data will help us determine who should receive treatment. Further information is also needed on the effect of laser iridotomy on eyes in the very earliest stages of angle-closure. Most of these low risk eyes will never suffer significant loss of vision from PACG. It is important to be sure that laser PI does not cause significant side effects (such as cataract) in a small number of people, that may outweigh its benefits in preventing a few cases of PACG. However, there is now considerable optimism that screening and prophylactic treatment for PAC and PACG may be a viable method of preventing blindness in very large numbers of people in Asia.
References
1 Salmon JF, Mermoud A, Ivey A, Swanevelder SA, Hoffman M. The prevalence of primary angle-closure glaucoma and open angle glaucoma in Mamre, Western Cape, South Africa. Arch Ophthalmol 1993; 111: 1263-1269.
2 Foster PJ, Baasanhu J, Alsbirk PH, Munkhbayar D, Uranchimeg D, Johnson GJ. Glaucoma in Mongolia – A population-based survey in Hövsgöl Province, Northern Mongolia. Arch Ophthalmol 1996; 114: 1235-1241.
3 Foster PJ, Oen FT, Machin DS, et al. The prevalence of glaucoma in Chinese residents of Singapore. A cross-sectional population survey in Tanjong Pagar district. Arch Ophthalmol 2000; 118: 1105-1111.
4 Hollows FC, Graham PA. Intraocular pressure, glaucoma and glaucoma suspects in a defined population. Br J Ophthalmol 1966; 50: 570-586.
5 Hu Z, Zhao ZL, Dong FT. [An epidemiological investigation of glaucoma in Beijing and Shun-yi county]. [Chinese]. Chung-Hua Yen Ko Tsa Chih [Chinese Journal of Ophthalmology]. 1989; 25: 115-118.
6 Clemmesen V, Alsbirk PH. Primary angle-closure glaucoma (a.c.g.) in Greenland. Acta Ophthalmol 1971; 49: 47-58.
7 Luntz MH. Primary angle-closure glaucoma in urbanized South African caucasoid and negroid communities. Br J Ophthalmol 1973; 57: 445-456.
8 Seah SKL, Foster PJ, Chew PT, et al. Incidence of Acute Primary Angle-closure Glaucoma in Singapore. An Island-Wide Survey. Arch Ophthalmol 1997; 115: 1436-1440.
9 Foster PJ, Alsbirk PH, Baasanhu J, Munkhbayar D, Uranchimeg D, Johnson GJ. Anterior chamber depth in Mongolians. Variation with age, sex and method of measurement. Am J Ophthalmol 1997; 124: 53-60.
10 Au Eong KG, Tay TH, Lim MK. Race, culture and myopia in 110,236 young Singaporean males. Singapore Med J 1993; 34: 29-32.
11 Johnson GJ. Myopia in arctic regions. A survey. Acta Ophthalmol (Suppl.). 1988;Suppl. 185: 13-18.
12 Quigley HA. Number of people with glaucoma worldwide. Br J Ophthalmol 1996; 80: 389-393.
13 Devereux JG, Foster PJ, Baasanhu J, et al. Anterior chamber depth measurement as a screening tool for primary angle-closure glaucoma in an East Asian population. Arch Ophthalmol 2000; 118: 257-263.
14 Foster PJ, Devereux JG, Alsbirk PH, et al. Detection of gonioscopically occludable angles and primary angle closure glaucoma by estimation of limbal chamber depth in Asians: modified grading scheme. Br J Ophthalmol 2000; 84: 186-192.
15 Seah SKL, Foster PJ. Anterior Chamber Depth Measurement Variation. Invest Ophthamol Vis Sci (ARVO Suppl). 1997; 38: S164(Abstract).
16 Nolan W P, Foster P J, Devereux J G, et al. YAG laser iridotomy treatment for primary angle closure in east African eyes. Brit J Ophthalmol 2000; 11: 1255-1259.