")
The increasing problem of retinopathy of prematurity
Related content
Background
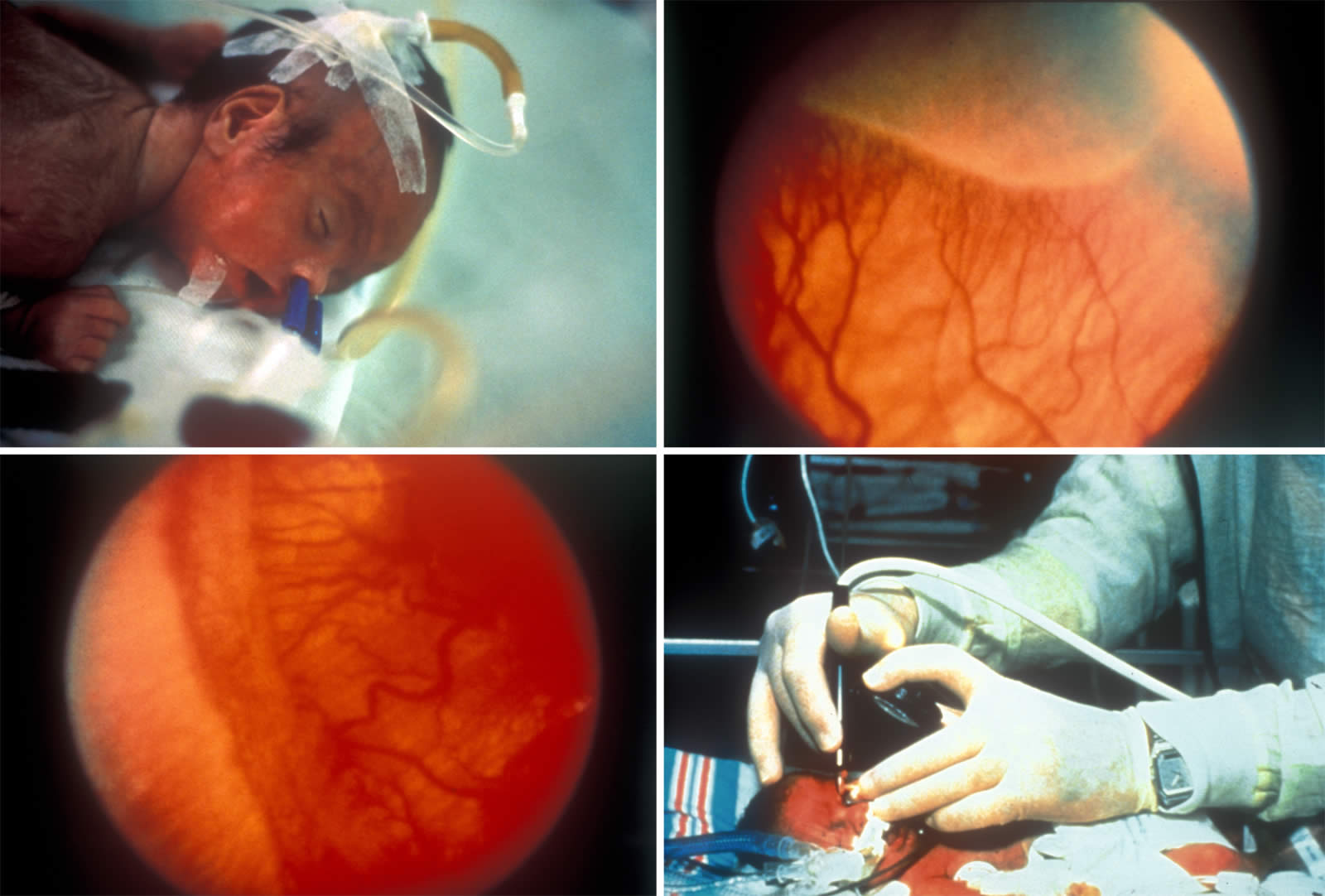
Retinopathy of prematurity (ROP) is an important cause of avoidable childhood blindness in industrialised countries. It is also emerging as a problem in economically developing parts of the world because of the ever increasing survival of low, and very low birth weight infants, especially in urban settings.
Many studies have investigated risk factors for ROP, and the major parameters are low birth weight and pre-term birth. In addition, the infant retina has been shown to be very susceptible to fluctuating oxygen levels. The development of ROP seems to be determined by the immaturity of the infantile retina and how early the damage to the tissues starts. Other factors related are hypoxia, septicaemia, acidosis, vitamin E deficiency and intraventricular haemorrhage.1
Table 1. Mortality rate/age < 1 year/ region (Brazil)
| Region | 0-6 days | 7-27 days | > 28 days | Total |
|---|---|---|---|---|
| North | 49.64 | 12.37 | 37.99 | 100 |
| Northeast | 39.71 | 10.87 | 49.42 | 100 |
| Southeast | 52.23 | 14.04 | 33.73 | 100 |
| South | 46.88 | 12.58 | 40.54 | 100 |
| Centre-west | 51.06 | 14.09 | 34.85 | 100 |
| Total | 47.11 | 12.66 | 40.23 | 100 |
Retinopathy of prematurity has been reported to be responsible for 4.1-38% of severe visual impairment/blindness (SVI/BL) in Latin America.2 Countries with intermediate infant mortality rates (10-60 per 1000 live births) seem to have the highest proportion of childhood blindness due to ROP. These are middle-income countries that are introducing or expanding intensive neonatal care services in private and government sectors. Surviving neonates are generally not screened or treated for ROP, thus increasing the prevalence of blindness and severe visual impairment. Industrialised countries have infant mortality rates of less than C0 per 1000 and good neonatal intensive outcomes. In these settings ROP accounts for 6-18% of childhood blindness.2 There is little data on the proportion of premature, low birth weight babies who have the different stages of ROP, as well as little data on the proportion of childhood blindness due to ROP in Brazil. As ROP seems to be associated with infant survival, these rates may reflect overall mortality rates for each region (Table 1). There is neither a national programme for ROP screening nor available official childhood blindness registration data. As an isolated initiative, some public and private institutions perform screening for ROP using different guidelines.
The data presented in this paper come from examining babies in one neonatal unit in Rio de Janeiro, Brazil over a 3-year period (1998-2000). The data have been extrapolated to estimate the number of babies at risk of ROP in Rio, and in Brazil as a whole. The implications for screening programmes in Brazil are discussed.
Recent Data from One Neonatal Unit in Rio de Janeiro, Brazil
The Fernandes Figueira Institute /Oswaldo Cruz Foundation (IFF/FIOCRUZ), Rio de Janeiro, is one of the national reference centres for maternal and infant care. Screening for ROP has been undertaken since 1998. Criteria for screening are a birth weight ofýless than or equal to 1500 g and gestational age less than 33 weeks. The first exam was performed 4 – 6 weeks after birth, and follow-up depended on the retinal findings at the time of each examination. Treatment by cryotherapy to the avascular peripheral retina was indi-cated when threshold disease was diagnosed.
Table 2. ROP stages/birthweight 1998-2000 (IFF)
| < 1000g Number |
< 1000g % |
1000 – 1500g Number |
1000 – 1500g % |
Total No. Screened Number |
Total No. Screened % |
|
|---|---|---|---|---|---|---|
| No ROP | 2 | 4 | 57 | 54 | 59 | 37.6 |
| ROP I | 7 | 14 | 22 | 21 | 29 | 18.5 |
| ROP II | 27 | 52 | 22 | 21 | 49 | 31.2 |
| ROP III | 5 | 10 | 3* | 3 | 8 | 5.1 |
| ROP III plus | 8 | 15 | 1* | 1 | 9 | 5.7 |
| ROP IV | 1 | 2 | 0 | 0 | 1 | 0.6 |
| ROP V | 2 | 4 | 0 | 0 | 2 | 1.3 |
| Total | 52 | 100 | 105 | 100 | 157 | 100 |
Data collected from all surviving premature infants born between January 1998 and December 2000 are shown in Table 2. Any stage of ROP was diagnosed in 62.4% and threshold disease in 7.3% of the 157 examined babies. The vast majority of babies needing treatment weighed <1,000g at birth, but 4 babies with birth weights of 1000-1210g developed Stage III or Stage III plus disease.
Extrapolation of Findings to Rio de Janeiro and Brazil
In order to determine the present situation in Rio de Janeiro County, data on all live births were collected for the year 2000 with the cooperation of the Municipal Secretary of Health. Rio de Janeiro has a population of approximately 5.6 million people, with 103,000 live births/year. It is estimated that 931 neonates with a birth weight less than 1500g survived to 6 weeks (survival rate of 62.7%) in the public hospitals, and required screening for ROP. Only 5 % of these 931 neonates are known to have been screened and treated (Table 3). There are no data for the private units, but it is estimated that around 202 neonates under 1500g survived in 2000. In the whole county in the year 2000, therefore, there were approximately 1133 babies at risk of ROP; approximately 60 – 80 babies would have required treatment, and up to 40 may have become needlessly blind.
Table 3. Number of live births in Rio de Janeiro City weighing < 1,500g from Jan-Dec 2000 and survival rates in the different public neonatal intensive care units
| Live births | Survivors | % Survival | |
|---|---|---|---|
| 9 County Hospitals | 925 | 604 | 65.3 |
| 3 State Hospitals | 185 | 101 | 54.6 |
| 3 FederalHospitals | 301 | 177 | 58.8 |
| 2 University Hospitals | 74 | 49 | 66.2 |
| Total | 1485 | 931 | 62.7 |
Brazil is a large country with huge regional variation in levels of socio-economic development, and a population of approximately 160 million people. It is estimated that of the 3 million live births in 2000, 1% have a birth weight of less than 1500g. Based on an overall mortality rate of 40%, there are estimated to be 18,000 survivors at risk of ROP each year, all of whom require screening for ROP. There is some variation in the proportion of babies with threshold disease, but it is likely that 5-7% of those at risk will benefit from treatment, i.e., 900 -1260 babies each year. If all these neonates were not screened or treated, 450 – 630 would become needlessly blind. Considered in terms of blind-years (i.e., number of individuals blind x estimated life expectancy), this translates to approximately 22,500 – 31,500 blind years annually. Blind babies have a lifetime of blindness ahead, with all the social, economic and emotional costs entailed.
Implications for screening
On increased incidence of blindness from ROP can be expected in Brazil, as services for neonates are being introduced. To prevent this, there is a need to promote some specific disease control measures, development of human resources as well as Qppropriate technology and infrastructure according to the Vision 2020 programme.3 There is an evident need to start a screening programme. To assure better communication among the involved group as well as awareness of the importance of screening, workshops about retinopathy of prematurity for all health care professionals, including neonatologists, nurses and social workers should be organised. Provision of adequate equipment is recommended as none of the units have an indirect ophthalmoscope or 28 D lens for diagnostic purposes, nor do they have cryo or laser devices for treatment. In addition, well trained ophthalmologists are required to perform indirect ophthalmoscopy in pre-term babies as well as treat threshold disease. However, hindrances in implementing a programme in an integrated fashion, with adequate planning, are predictable in such a large country as Brazil. According to Ziakas et al, a co-ordinated regional strategy can improve the implementation of national guidelines for screening ROP, which in the UK resulted in a higher uptake for babies most at risk.4 Screening guidelines pertaining to industrialised countries may prove inappropriate in middle-income economies, which may have lower standards of neonatal care and poorer neonatal outcomes. In these situations larger, less pre-term babies who might be at risk of ROP would not be included in a screening programme. Since 2001 a new protocol has been adopted, which was developed by the NO-ROP GROUP. The establishment of new programmes throughout Latin America provides an excellent opportunity to collect data from all the countries involved using standard screening criteria, examination methods and definitions of disease. The new screening criteria are birth weight less than 1750g and all who have had 30 or more days of oxygen, regardless of birth weight or gestational age. The first examination should be at 6 – 7 weeks after birth. Blindness and visual impairment have important socio-economic implications. Blindness occurring in infancy is a long-lasting burden, both in terms of social dependence and lost productivity. Therefore, a public health intervention that saves the sight of even a relatively small number of infants and children provides significant savings, while ensuring a better quality of life for those affected.
Ackowledgments
The author would like to express her gratitude to Dr Clare Gilbert and Dr Allen Foster for their advice.
References
1 Gilbert C. Retinopathy of Prematurity: Epidemiology. J Comm Eye Health 1997; 10: 22-24.
2 Gilbert C, Rahi J, Eckstein M, OSullivan, J, Foster A. Retinopathy of prematurity in middle-income countries. The Lancet 1997; 350: 12-14.
3 Gilbert C, Foster A. Bull WHO 2001; 79(3): 227-232.
4 Ziakas NG, Cotrell DG, Milligan DWA, Pennefather PM, Bamashmus MA, Clarke MP. Regionalisation of retinopathy of prematurity (ROP) screening improves compliance with the guidelines: an audit of ROP screening in the Northern Region of England. Br J Ophthalmol 2001; 85: 807-810.