")
The maintenance and repair of ophthalmic surgical instruments: training at the eye clinic
Related content
Introduction
Ophthalmic microsurgical instruments are delicate and require special care. In developing countries, where instruments are usually difficult to replace, maintenance and repair are even more important. The Jan Worst Research Group started a project in 1994 – after several requests for assistance in the repair of ophthalmic microsurgical instruments – to train staff at eye clinics to maintain and repair these instruments.
Objectives
The objectives of this project were the following:
- Development of simple techniques to maintain and repair surgical instruments in different settings
- Assembly of a toolbox with all necessary tools, instruments and consumables to perform the maintenance and repair techniques
- Production of training and reference materials
- Train staff at eye clinics in the maintenance and repair of surgical instruments.
Methodology
Training
Training was designed for ophthalmic and technical staff in eye clinics in different hospital settings in several countries in Africa and Asia. It was decided to have training on site rather than in a central place in the country. This way more people from one clinic could be trained. In addition, this would provide the possibility of giving assistance in overcoming any initial or specific problems of a certain clinic. Further, more instruments would be available to give the staff trained more ‘hands on’ training in the techniques, using instruments from their own clinic.
Toolbox
A toolbox was assembled with all necessary tools to repair instruments and to manufacture some consumables. These tools included different sharpening stones, files, pliers, needle bending pliers, soldering equipment and lens cleaning cloths with enough consumables to last the clinic for at least one year. For sustainability reasons, the tools were good quality so they would not break down. Each clinic received a toolbox with the tools and instruments which are necessary to carry out the techniques on maintenance and repair of instruments.
ITIR, Manual & Video
Together with the Intermediate Technology Information Ring (ITIR), the manual on Appropriate Technology in Ophthalmology was revised in 1996. This manual was used as a reference manual for the clinics visited. A detailed video on maintenance and repair was produced for training purposes by the Jan Worst Research Group and the ITIR. With support of the Fred Hollows Foundation, a comprehensive manual to accompany the video was written as well. The video is available in English and French as VHS videotape and Video CD (mpeg) and the manuals in English as hardcopy or pdf file
Editor: For further information about these training materials, contact Dr Danny Haddad at the address given above or by email to [email protected]
Clinics
In each country where the project took place an average of four clinics were visited. An introduction was given to the ophthalmologists of the clinics, with further in-depth training of theatre nurses and/or hospital technicians. During the project, 31 clinics in nine countries (Ghana, Zimbabwe, Malawi, Tanzania, Kenya, Uganda, Ethiopia, Papua New Guinea and Nigeria) were visited. The hospitals were a mixture of teaching, provincial and mission hospitals.
Workshops
Workshops were conducted in both Lao PDR and Vietnam, with participants from six and nine clinics respectively. Due to limited time the workshops in these countries were performed at a central place rather than visiting all the separate clinics.
Techniques taught and used
To understand what is wrong with an instrument, its way of functioning has to be understood. This included the testing of instruments to see if they were working properly or malfunctioning.
Cleaning instruments
The importance of good cleaning of instruments was stressed, especially in regard to rust prevention and sterility when using liquid sterilisation. Correct ways of cleaning were demonstrated, using mild soaps and gauze.
Maintenance of equipment and instruments
Maintenance of ophthalmoscopes and slit-lamps was included in the training sessions after clinics reported this to be a major problem. The most common problem was accumulation of dust on lenses.
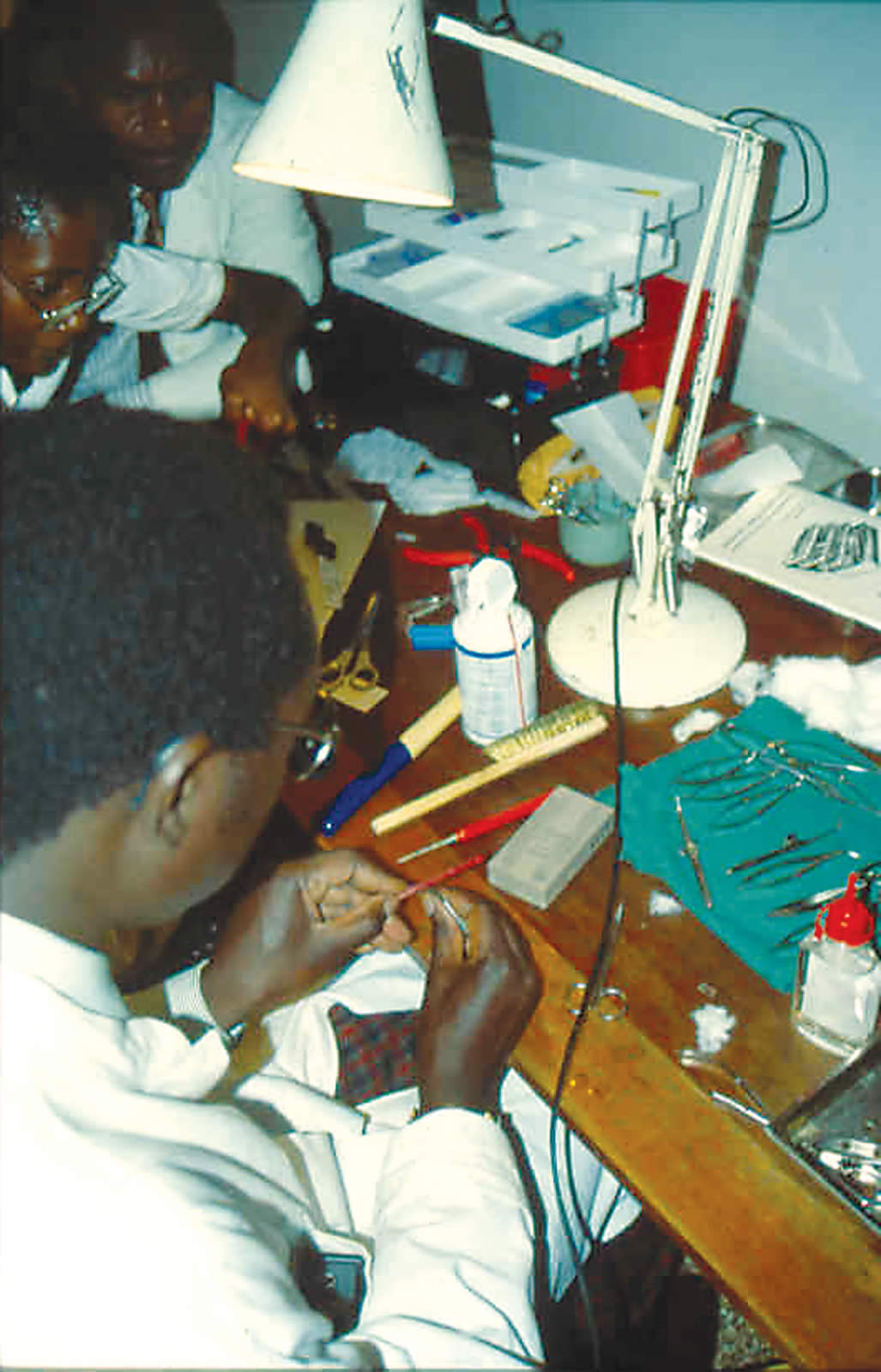
Repair of surgical instruments
The most important technique was sharpening of scissors. A small and very fine sharpening stone was included in the toolbox to sharpen ophthalmic surgical scissors. Most of the clinics visited had a box with non-functioning scissors, which were mostly blunt. Other techniques included were repair of worn out needle holders and forceps.
Manufacturing of consumables
Depending on the needs of the clinic, manufacturing of consumables was taught. The consumables offered included 8-0 silk sutures, surgical knives (using non-breakable razor blades) and cryo-extractors.
Lessons learned
Visiting separate clinics versus workshop in a central place
At the start of the project it was decided to visit the separate clinics instead of performing one workshop at a central location, although this had a major time implication. It was possible to set up the project in this way, since volunteers performed all the projects. With the experience in Lao PDR and Vietnam, both ways could be compared. In the authors’ view the visit to clinics had better results because there was time to give the trainees enough ‘hands on’ training and enough instruments were available for practice under guidance. During the workshop approach there were too many participants to give appropriate supervision during the practical sessions. Further, most clinics visited had specific problems which we were able to address during the visit.
One of the technicians who was trained had already received training in repair of instruments abroad. This technician complained that upon return it was not as easy as was shown during the training session.
Training of hospital technicians versus training of theatre nurses
In clinics where technicians were available, both technicians and theatre nurses were trained. Some clinics, with rotation of the nurses between theatre, OPD and the wards, wanted to have all nurses included. For these groups more general sessions were held with in-depth training for a few nurses – to become the experts in the clinic. In some of the teaching hospitals it was found that the technicians were too busy with work in the other departments to find free time to assist in the eye department. The most successful was the training of technicians in specialised eye hospitals like the National Eye Centre in Kaduna and the ECWA Eye Hospital in Kano, both in Nigeria.
Training versus donation of tools with training guides
Several of the clinics visited had received sharpening devices. Most of these came with instruction manuals and/or videos. However, the techniques were still found to be complicated and not fully understood and the sharpening devices were not utilised.
Conclusion
In the opinion of the authors it is very important to provide training for technicians and/or nurses in the maintenance and repair of microsurgical instruments in theatre and OPD. All clinics visited had a large number of instruments which were either blunt or broken. During training it is important that the participants receive enough experience through practical training. Providing training in their own clinic gives the participants the possibility of performing repair on their own instruments and in their own setting. Donating repair sets without the appropriate training gives poor results, since most training manuals and videos are still too complex.
The importance of regular maintenance should be stressed as this will often prevent the development of defects in equipment or instruments. A record of maintenance and of items repaired should be kept. This is particularly appropriate for larger items of equipment and, for example, surgical cataract sets.
It will be helpful if each clinic has a person recognised as responsible for maintenance, who will also keep maintenance records and make sure that regular maintenance is carried out.