")
What’s new in primary open angle glaucoma?
Related content
Primary open angle glaucoma (POAG) involves a spectrum of disorders typified by a characteristic optic neuropathy and field loss in eyes with open drainage angles. It is currently a leading cause of blindness worldwide, and in the future should become every more important as populations age throughout the world. Recently, we have witnessed a number of exciting advances in glaucoma. Developments have occurred regarding diagnosis, treatment, genetics and the relationship of intraocular pressure (IOP) to disease progression.

Recent new findings
A. Diagnosis
Optic nerve and retinal nerve fibre imaging
Limitations in optic disc and retinal nerve fibre layer assessment have stimulated the development of imaging devices “hat measure either the optic disc cup and neuroretinal rim area or the retinal nerve fibre layer. The most advanced at present are scanning laser tomography (Fig.1) and scanning laser polarimetry (retinal nerve fibre analyser). They offer greater objectivity but are limited by potential sources of error and so the results must still be interpreted in association with clinical findings. This quantitative imaging may be useful in early diagnosis before obvious visual field loss occurs and may allow increased sensitivity to detect progression of the condition.
Visual field and psychophysical testing
New fast test visual field strategies, such as SITA Swedish Interactive Thresholding Algorithm), have become available which improve patient test compliance. omputerised programmes for serial visual field analysis (PROGRESSOR), which assess progression of disease by accounting for test variability are available. Other modes of testing which involve motion detection may enable earlier diagnosis.
B. Treatment
Medical
The introduction of sustained release, once a day form of b blocker or pilocarpine has proved useful in terms of better compliance and convenience. However, prostaglandin analogues, which increase uveoscleral outflow, have had the most significant impact. Latanoprost (Xalatan) appears to be the most effective IOP-reducing agent currently available, with a low incidence of ocular and systemic side effects. Unoprostone (Rescula), Bimatoprost (Lumigan) and Travoprost (Travatan) have all recently been approved for use by the Food and Drug Administration in the United States.
Opical carbonic anhydrase inhibitors, such as Dorzolamide (Trusopt), lower IOP but less effectively than oral acetazolamide. Another form, rinzolamide (Azopt) has a more physio-logic pH and so less topical side effects. The alpha agonist, Brimonidine OAlphagan) is claimed to be neuroprotective, but no clinical evidence exists.
Surgical
One of the most fundamental questions in glaucoma, ‘How low must the IOP be to prevent further glaucoma damage?’ has recently been addressed by a multicentre, prospective clinical trial.1 Patients with advanced POAG and IOP consistently less than 18 mmHg after surgery (mean IOP 12.3 mmHg) were found to have no visual field progression after 8 years of follow up. The clinical implication is that we should aim for a low normal target IOP range in patients with moderate to severe glaucoma.
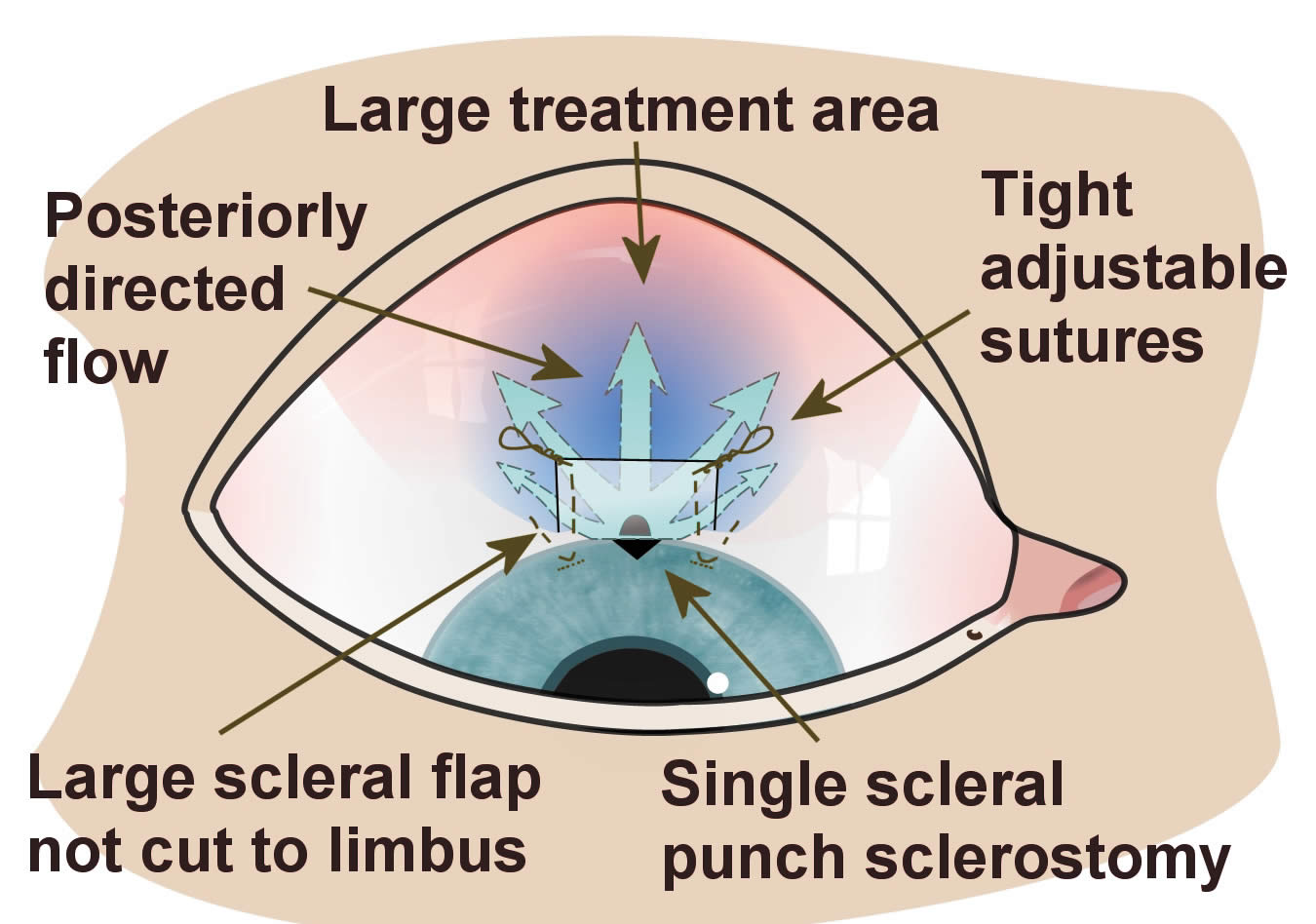
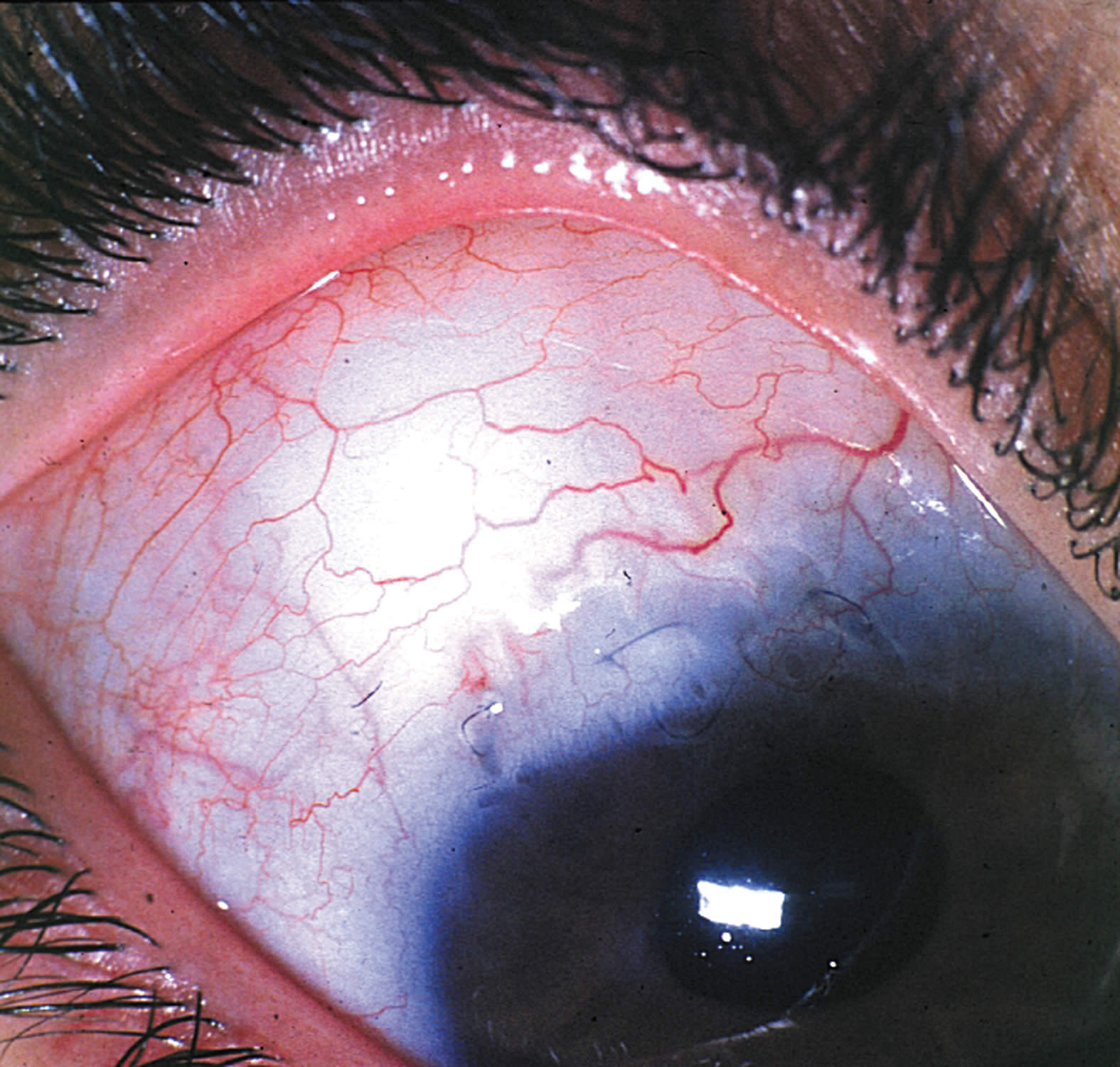
The use of the antimetabolites, 5-Fluorouracil (5FU) and Mitomycin-C (MMC), to prevent surgical failure has been the greatest advancement in glaucoma surgery over the last two decades. Single, intraoperative applicationBhas improved convenience of drug delivery. Strategies that change bleb morphology favourably are now available to avoid the development of focal, thin, avascular cystic blebs associated with antimetabolite use. These include a larger surface area of antimetabolite treatment,2 a fornix based conjunctival flap to reduce posterior restriction and a large scleral flap with closure that diverts aqueous posteriorly (Fig. 2). These simple modifications can achieve a much more diffuse, non-cystic bleb even with high dose antimetabolites (Fig. 3).
Recently, there has been renewed interest in non-penetrating trabecular surgery because of the desire to avoid potential complications associated with ocular entry, such as hypotony and subsequent cataract. Although prospective, comparative studies of these new methods with trabeculectomy have demonstrated fewer complications, it has become evident that non-penetrating surgery is not as successful in reducing IOP.3 However, a higher incidence of cataract formation following trabeculectomy may in fact entirely reduce this advantage.
C. Genetics
Our understanding of the genetic basis of glaucoma has improved considerably over the past decade. It is likely that the aetiology of POAG is multifactorial 4 resulting from a combination of mutations in more than one gene and as yet unidentified environmental factors. With regard to juvenile and adult-onset POAG, several loci have been identified. However, only one gene is known, namely the myocilin / TIGR (trabecular meshwork inducible glucocorticoid response) gene at the GLC1A locus on chromosome 1q21-q31. More than thirty mutations of this gene have been identified in ethnically diverse populations worldwide. Studies have shown that it is responsible for only about 5% of POAG overall.
Research issues
Although impressive advancements have occurred in glaucoma, the future appears to be even more exciting.
A. Diagnosis
Another scanning device currently being developed is 3rd generation optical coherence tomography with ultrahigh resolution (2-3 mm). It allows in vivo visualisation of retinal structures and may prove useful for early diagnosis. Similarly, $ultifocal visual evoked potentials (mVEP) objectively may identify visual field defects earlier than white on white perimetry.
B. Treatment
Medical
As the role of IOP-independent mechanisms becomes increasingly recognised, innovative treatments include agents that improve ocular blood flow or are neuroprotective. Furthermore, the possibility of a ‘medical trabeculectomy’ based on biochemical and genetic manipulation of the trabecular meshwork to restore function is very exciting as is work on trabecular meshwork cell transplantation.
Surgical
The healing process is the main determinant of IOP following glaucoma filtration surgery. The ongoing search for safer, less toxic and more effective antiscarring agents has led to a number of exciting developments. Transforming growth factor b (TGF b), a potent stimulator of healing, can be successfully neutralised in vivo and in vitro with humanised antibodies and studies are currently underway to assess clinical efficacy. Ultimately, other specific agents may allow us to set the IOP safely after surgery in the 10-14 mmHg range.
C. Genetics
The transmission of disease in GLC1A families is autosomal dominant with variable penetrance. Presymptomatic diagnosis of at risk individuals in pedigrees with GLC1A mutations is already possible. But, as the mutation is responsible for a small fraction of POAG, the most useful role of screening will be in large families with early onset, severe disease where early diagnosis and intervention may improve prognosis and also allow for genetic counselling. Hopefully, a greater understanding of basic genetic biology will identify patients at risk and ultimately lead to new treatments that prevent or cure the disease.
VISION 2020
The main problem continues to be identifying patients who are in need of intervention, particularly individuals in developing countries who account for 85% of patients affected with glaucoma. In the industrialised world, only 50% of people with established POAG are diagnosed, usually through the course of routine eye examination. But in the developing world, patients frequently present with severe visual loss before they are identified. However, screening a population for a rare disease such as glaucoma is difficult, especially when the infrastructure to deal with positive cases is lacking. To achieve the Vision 2020 goals to reduce blindness from glaucoma in developing countries, we need strategies that identify individuals with obvious glaucoma, using simple tests. Detection rates can be increased by improving the training of staff in optic disc, IOP and visual field examination and also by increased public awareness of the potential benefits of regular eye examination.
Currently, glaucoma filtering surgery with adjunctive anti-scarring therapy offers the best single intervention strategy to slow the rate of disease progression by sufficiently lowering IOP to prevent blindness. The challenge will be to deliver this in a form that is relatively simple, safe, fast and inexpensive with an acceptable long-term success rate. Given what we now know, this may soon be possible.
Acknowledgements
We are grateful to the Medical Research Council (G9330070), the International Glaucoma Association and Moorfields Trustees who are supporting our glaucoma and wound healing research programme. We would also like to thank Mr Alan Lacey for his help with the diagrams.
References
1 The advanced glaucoma intervention study (AGIS) 7. The relationship between the control of intraocular pressure and visual field deterioration. Am J Ophthalmol 2000; 130: 429-440.
2 Cordeiro MF, Constable PH, Alexander RA, Bhattacharya SS, Khaw PT. Effect of varying the mitomycin-C treatment area in glaucoma filtering surgery in the rabbit. Invest Ophthalmol Vis Sci 1997; 38: 1639-1646.
3 Chiselita D. Non-penetrating deep sclerectomy versus trabeculectomy in primary open angle glaucoma surgery. Eye 2001; 15:197-201.
4 Budde WM. Heredity in primary open angle glaucoma. Curr Opin Ophthalmol 2000; 11: 101-106.