")
Eye in primary health care teaching set. Full text
1. The normal eye and tarsal conjunctiva

On the left you see a normal eye. The eyelashes point outwards and the eyelids will open and close easily. The white part of the eye, the sclera, with the overlying conjunctiva, is not red and inflamed. The cornea is bright and clear. The pupil is black and round. If the pupil and iris are well seen, this confirms that the cornea must be clear.
Now look at the normal everted eyelid shown on the right: it is pink and the small blood vessels are clearly visible. The surface, which is also conjunctiva, is smooth.
Examine the normal eyes of your friends so that you can recall how healthy eyes should appear on examination!
2. Anatomy of the eye
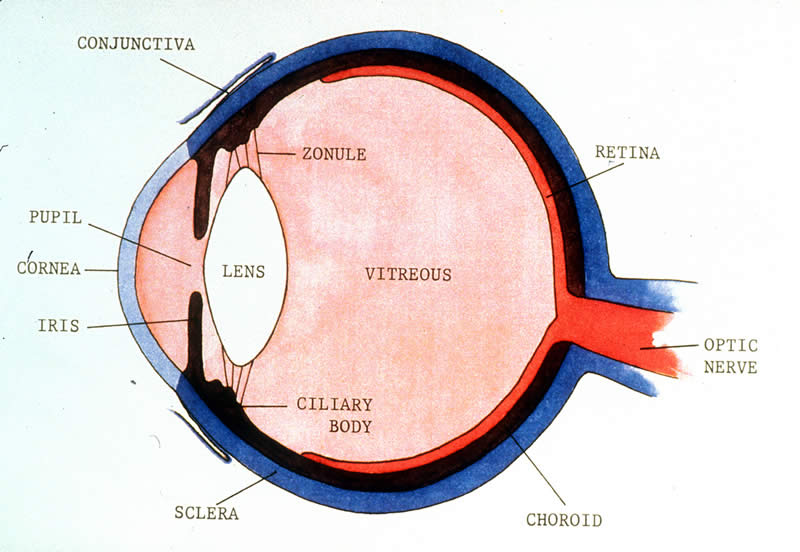
This picture shows a diagrammatic cut section of a normal eye.
The main protective outer coat of the eye is the sclera. Overlying the front part of the sclera is a thin membrane, the conjunctiva. At the front of the eye there is a round clear area, the cornea, which allows light to enter into the eye. The cut section shows that the eye has the form of a balI. The light passes through the cornea and the lens to the retina at the back of the eyeball. The retina consists of light receptors and nerves which send messages to the brain through the optic nerve. The amount of light entering the eye can be regulated by changes in the iris. If the iris contracts, the pupil becomes small and little light can enter. If the iris relaxes, the pupil becomes wider and more light is allowed to enter (for example at night).
There are different reasons why people with eye problems will come to you for help. Those with sudden onset of pain in the eye, or sudden loss of vision, come for treatment much earlier than those who have no pain and whose vision is getting worse over a long period of time. Most ‘sudden onset’ eye problems also require quick action.
We shall start with sudden (or acute) eye problems.
Ask about the onset of the complaint and how the condition has progressed, together with information on personal and family health.
A careful examination beginning with the visual acuity of each eye, then a general impression of the patient and the appearance of both eyes together, followed by examination of each eye on its own, gives an ordered approach which should not miss any important details. Begin with the front of each eye and then examine deeper structures:
- eyelids
- conjunctiva and sclera
- cornea
- anterior chamber, iris, pupil and lens
- optic nerve and retina (if you have an ophthalmoscope)
You should try and make a diagnosis, and decide whether to treat the patient or refer to an eye specialist.
3. Corneal foreign body
This patient had acute onset of pain in the eye. On examination, you can clearly see a foreign body on the cornea. Usually, a patient will remember the exact time when a foreign body entered the eye. Severe pain of sudden onset and a watering eye is characteristic of a corneal foreign body.
How do you manage a foreign body on the cornea?
First, see if the foreign body lies on the surface, or deeper in the cornea. If it lies on the surface, wash it off or gently wipe it off with a wet cotton tip, then apply an antibiotic eye ointment and ask the patient to come for review the following day. If the foreign body cannot be removed easily, or lies deeper in the cornea, do not try to remove it – give antibiotic eye ointment, pad the eye and refer the patient for further treatment at the hospital or eye clinic.
If you cannot see a foreign body, always evert the upper eyelid to see if it lies under the eyelid.
To summarize – if a foreign body lies superficially:
1. Lie the patient flat.
2. Give local anaesthetic eyedrops
3. Use a good light.
4. Lift off the foreign body.
4. Corneal abrasion and chemical injury
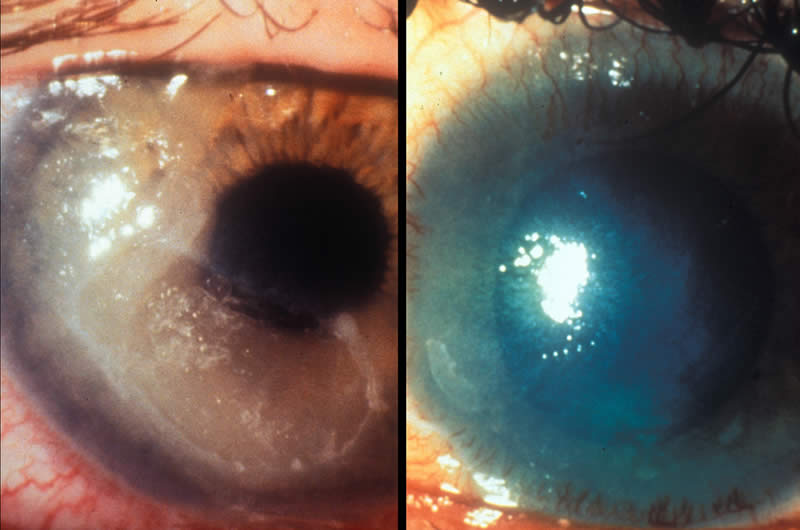
Sometimes a patient presents with symptoms of a foreign body but you cannot find a foreign body. You may note that the surface of the cornea is not smooth and shiny – there are scratches – a corneal abrasion. The picture on the left shows a large corneal abrasion. This can be easily caused – for example, the thumbnail of a child may scratch a mother’s eye. The eye is painful, red and watering. You may use a local anaesthetic eyedrop to ease the pain during your examination. Fluorescein dye – applied either in single drop form (minims) or a paper strip applicator – will outline the extent of the abrasion. In this case give an antibiotic eye ointment, apply a firm eye pad and a bandage so that the eyelids are closed over the front of the eye. Check the patient again the following day. Large abrasions may need a pad and bandage for a further 24 hours. Again apply antibiotic
If the eye is not better after 3 days, refer for further advice and treatment.
If chemicals spill into one or both eyes the patient will complain of pain, watering and often blurring of vision.
On examination you may see a cloudy cornea as shown in the picture on the right.
If a patient comes to you with a history of chemical injury to the eye, you must not waste any time. This is an emergency!
Wash the eye IMMEDIATELY with water – if necessary for up to 15 minutes. Make sure that the eyelids are open to allow the water to dilute the chemical and to wash it off the cornea and conjunctiva in all areas, including under the eyelids. All solid particles must also be removed. Apply antibiotic eye ointment after washing. It the cornea is not clear after washing, refer the patient immediately for further medical treatment.
Do not use any medicines containing steroids.
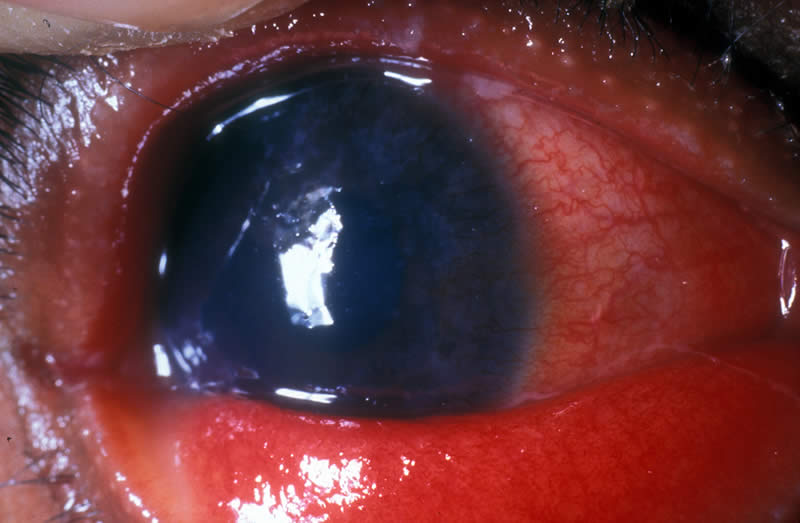
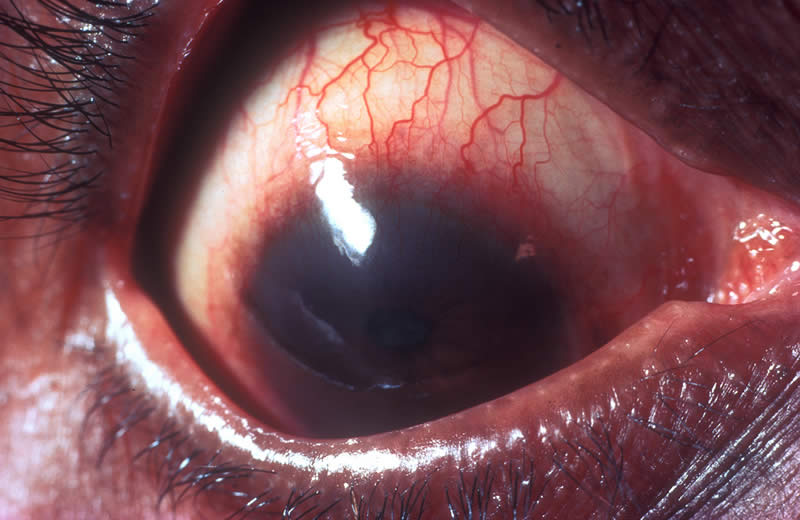
5. Penetrating eye injury
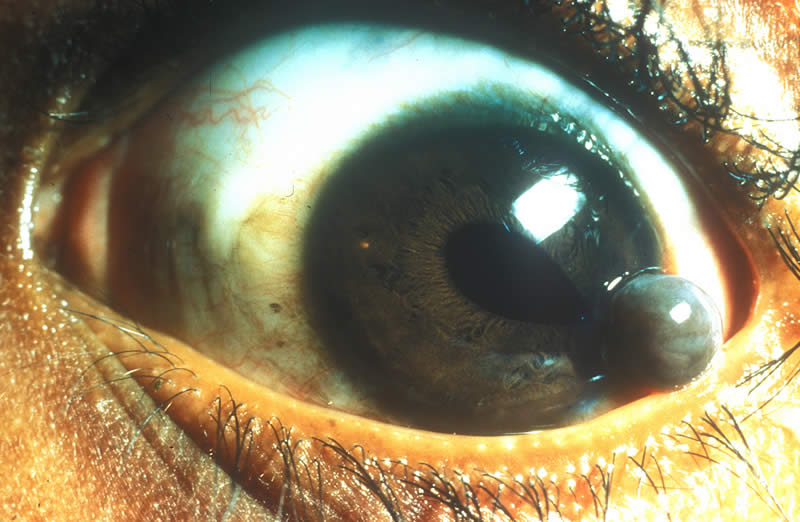
What has caused this unusual appearance of the front of the eye?
There has been a penetrating wound of the cornea and black tissue is coming through the wound. The eye was hit by a sharp object. There will be varying degrees of pain and poor vision. Here the eye is remarkably ‘quiet’ – more inflammation is usually present. Some time has passed since the injury, which was caused by a thorn. Iris tissue is presenting through the corneal wound. This is a serious situation.
Apply an antibiotic eyedrop or, if this is not available, eye ointment. Secure a sterile protective shield over the eye, without touching or pressing on the eyeball, and refer the patient immediately to a specialist.
The patient should remain as quiet as possible until seen by the eye specialist. Surgery will be required.
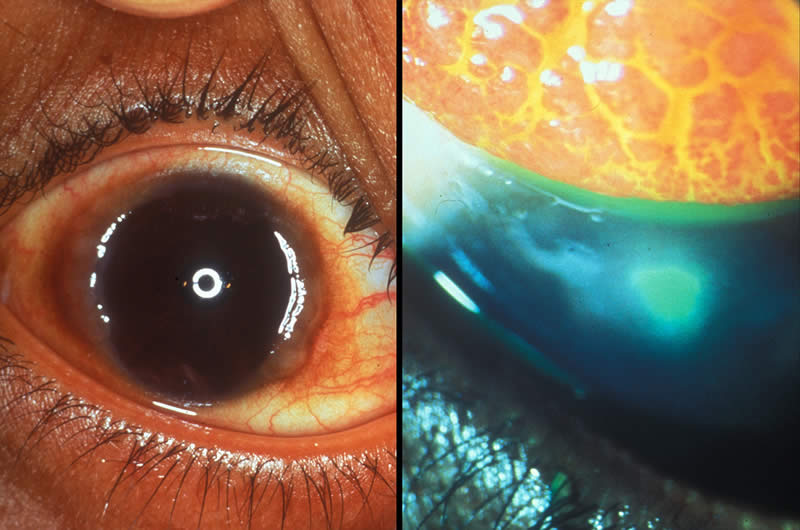
6. Blunt eye injury

What can you see in these two pictures?
The picture on the left shows blood on the white part of the eye. This is a subconjunctival haemorrhage – blood under the conjunctiva.
In the case of a subconjunctival haemorrhage there is no loss of vision or pain. In older patients a subconjunctival haemorrhage may occur without injury. You do not have to give any treatment for an isolated haemorrhage. After two or three weeks the haemorrhage will have disappeared.
In the picture on the right, there is blood behind the cornea, inside the eye. The iris has been bleeding. Blood behind the cornea and in front of the iris is called an hyphaema. This may cause a rise in intraocular pressure and the further complication of corneal blood staining.
In both of these cases, however, the patient will often tell you that he was hit on the eye, perhaps by a fist or a ball or that he was involved in some other accident.
In the case of a small hyphaema the patient must stay in bed for 5 days. If pain is severe, if some blood is still present in the eye after 5 days or if the vision is still reduced after the hyphaema has gone then you should refer the patient for specialist advice. If the hyphaema is total, filling all the area behind the cornea, refer immediately – this blood must be removed surgically otherwise there will be a rise in intraocular pressure with corneal blood staining and possible long-term loss of vision.
Aspirin can increase bleeding, so do not give aspirin to these patients.
Sections 3, 4, 5 and 6 have discussed different types of injury to the eye, their diagnosis and management:
- Foreign bodies
- Corneal abrasions
- Chemical injuries
- Penetrating injuries
- Blunt injuries
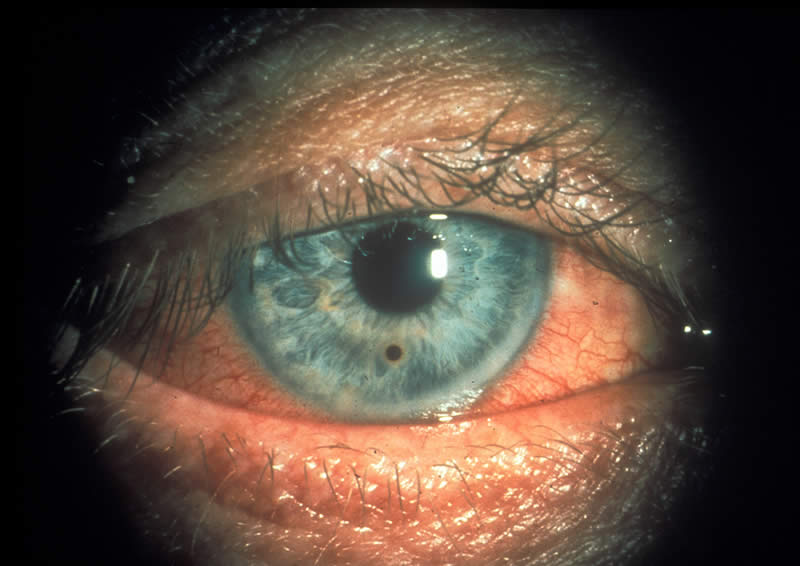
7. Ophthalmia neonatorum

What is the age of this patient? What do you notice about the eyes?
The baby is less than four weeks old and has a very severe purulent conjunctivitis – this is newborn conjunctivitis or ophthalmia neonatorum. This type of conjunctivitis starts soon after birth because the baby was infected by the mother during delivery. The mother already had an infection of the vagina due to the presence of a sexually transmitted disease, in this case gonorrhoea.
On examination you can see that both eyes are red and there is a lot of purulent discharge. Be careful because the pus is infectious! Wash your hands carefully after your examination. You must clean the eyelids and eyes with water and swabs and then apply tetracycline 1% eye ointment every hour until there is improvement. Arrange for referral to the eye specialist.
The child will need at least one antibiotic injection and possibly more than one, depending on the antibiotic used. If the cornea is not clear due to involvement in the infection then this is a very serious disease and you must immediately refer the baby for specialist opinion.
Advise both parents to seek medical treatment for the sexually transmitted disease which probably affects the father as well as the mother.
Ophthalmia neonatorum may be caused by a number of different organisms, but the most common are Chlamydia Trachomatis and Neisseria Gonorrhoeae.
You can prevent this disease by immediately cleaning the eyelids of newborn babies with a clean cloth and water and applying tetracycline 1% eye ointment. Every newborn baby should be treated in this way by the midwife or nurse.
8. Viral conjunctivitis

What can you see in this eye?
The eye is red – the conjunctiva is inflamed. The patient complains of irritation, redness and sometimes watery discharge. On examination you note that the white part of the eye (often both eyes) is red and there are many small conjunctival haemorrhages. This is epidemic haemorrhagic conjunctivitis,
What should you do?
An antibiotic eye ointment may be given three times daily to prevent secondary bacterial infection and to reassure the patient that he is being treated. Teach the patient or a relative how to do this.
At all times watch that the cornea remains bright and clear – if it becomes hazy, refer to an eye specialist. The infection is usually self-limiting and lasts for 5-14 days. Usually there are no longer-term complications.
It is very important to teach the patient not to rub his eyes and for the patient and relatives to wash their hands after touching the eyes. This can help to reduce spread of the infection.
9. Measles and the eye
Another example of an acute red eye caused by a virus is seen in this picture.
This is measles.
The measles virus is present in the corneal epithelium and conjunctiva and, in this child, there is both a measles keratitis and a conjunctivitis. An antibiotic eye ointment three times daily is given to prevent secondary bacterial infection and also to protect the eye. A vitamin A capsule, 200,000 IU, should be given especially if the cornea is hazy, and the dose is then repeated on the 2nd day and again after 1 to 4 weeks. The association between measles and vitamin A deficiency causing corneal ulceration and blindness is well recognised. Vitamin A deficiency will be further discussed in the next section. The general condition of the child should be treated as required.
10. Vitamin A deficiency and the eye
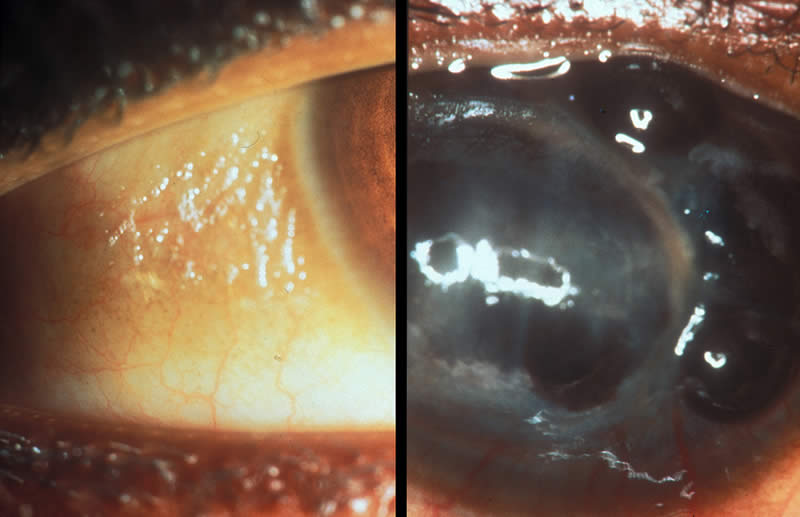
The eye on the left shows an early stage of xerophthalmia (vitamin A deficiency affecting the eye). You can see the white foam-like area on the lateral conjunctiva. This is called a Bitot’s spot. A patient with this condition is usually a child. Ask if the child can see at low levels of light. Look at the general condition of the patient. Very often these children are poorly nourished.
You can treat this patient and prevent more serious eye disease affecting the cornea by giving the child vitamin A, 200,000 IU immediately, another dose of 200,000 IU after one day and the third dose after 1 to 4 weeks. For a child less than one year of age, give 100,000 IU immediately, another dose of 100,000 IU after one day and the third dose after 1-4 weeks.
The cornea in the picture on the right is severely damaged.
Can you describe what has happened?
The cornea is irregular and ulcerating. A child with this appearance of the eye may be obviously malnourished or may have recently had measles infection or severe diarrhoea.
This child, in fact, had measles. The nutritional state of the child is poor. This is keratomalacia – a sudden softening of the cornea. It is the final stage of xerophthalmia, caused by lack of vitamin A in the diet.
Do not waste any time! You may be able to save some sight in a recently affected eye and at the same time protect the other eye. Give one capsule of vitamin A orally, 200,000 IU immediately. If the child is under one year of age, give
Apply an antibiotic eye ointment and use a protective eye shield. NEVER use any steroids. Then refer the patient immediately for further treatment. If that is not possible, give another 200,000 IU of vitamin A the following day and again after 1 to 4 weeks.
In this teaching set we are only referring to eye problems caused by a lack of vitamin A, but other serious diseases such as respiratory infections and diarrhoea may be associated with vitamin A deficiency and may threaten life. The general condition of the child should always be considered.
Certain foods are rich in vitamin A. These include dark green vegetables (such as spinach), also mangoes, papaya, carrots, and red palm oil. Even better sources of vitamin A are animal products, such as meat (liver), fish, milk and eggs. Vitamin A rich foods must be eaten regularly to prevent blindness in children due to xerophthalmia. Growing and eating of these foods should be encouraged. If these foods are not available or too expensive, vitamin A orally, 200,000 IU, can also be given, once every 4 to 6 months, to children aged 1 to 6 years of age. Children aged 6 to 12 months can be given 100,000 IU every 4 to 6 months, and children younger than 6 months 50,000 IU 3 times, 1 month apart. Within 6 weeks after delivery, women should be given 2 doses of 200,000 IU, one or more days apart.
Breast milk contains vitamin A and so young babies on breast milk do not need any extra vitamins. As soon as they need additional food, when weaning begins, it is very important that they are given enough vitamin A in their diet.
11. Herpes simplex and the eye
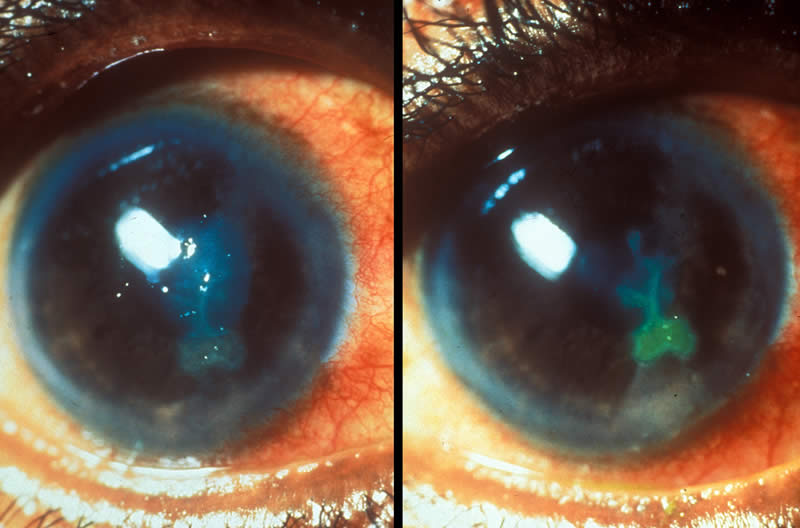
This is a special type of corneal ulcer caused by the virus Herpes Simplex. There is no pus or discharge.
The picture on the left shows a typical ulcer as you might first see it.
On the right the ulcer is stained with fluorescent dye and this outlines the typical branches with the colour green.
The patient may complain of pain, especially in strong light, and there is some loss of vision. There is watering and the eye is red. Usually only one eye is affected.
Treatment requires specialist care and therefore you must refer the patient urgently to an eye clinic or hospital. You can give an antibiotic eye ointment as protection against secondary bacterial infection.
NEVER give any steroids. Steroids will make the infection much worse.
12. Corneal ulcer
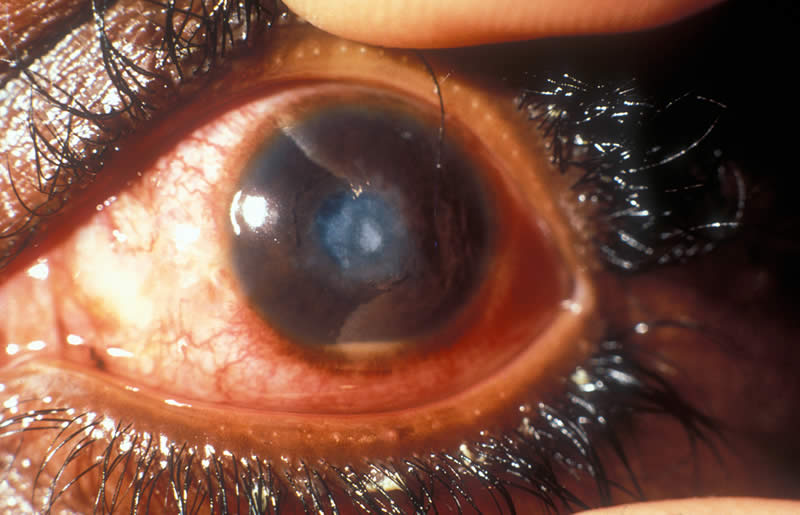
This patient presented with a history of pain in the eye and loss of vision.
On examination you see a red eye, and there is a white patch on the cornea. The surrounding cornea is hazy. There is pus inside the anterior chamber behind the cornea and in front of the iris (hypopyon).
This is a severe corneal ulcer, probably due to bacteria (or possibly a fungus).
How should you treat this eye?
Apply antibiotic eye ointment intensively, protect the eye with a shield and refer the patient immediately for further medical care. This patient will require further topical antibiotics and injected subconjunctival antibiotics, if it is confirmed that this is a bacterial infection.
NEVER give any eye ointment or drops containing steroids.
13. Iritis

What do you see in this image?
The eye is red and the view of the iris is slightly hazy – this is due to proteins and celIs circulating in the aqueous fluid in front of the iris. The pupil margin is irregular – there are inflammatory adhesions between the pupil margin and the anterior lens surface. These are called posterior synechiae.
Your patient will probably complain of pain and blurred vision.
Inflammation of the iris (iritis) is often associated with inflammation of the ciliary body (cyclitis), together described as iridocyclitis. This inflammation may be due to local causes or the presence of a systemic disease. For example, it can be associated with tuberculosis or onchocerciasis.
Treatment with anti-inflammatory medicine and dilating eye drops should be given.
Referral to the eye specialist is necessary.
14. Glaucoma
This patient comes to you with a typical history. A severe and deep pain developed in one eye and soon the patient could not see clearly. A severe headachewas present. Sometimes the patient may feel sick.
If you were asked to examine this eye, which findings would you note?
The eye is red, but you cannot see any pus. The cornea itself is not bright and clear. The surface looks hazy and slightly irregular instead of smooth and shiny. This is clue to corneal oedema.
This is acute glaucoma, a very serious condition, caused by high pressure inside the eye. Although not evident in this eye, the pupil is often dilated and not quite circular when compared with the other eye. If you place your two index fingers gently on the upper eyelid with the patient looking down and feel the eyeball through the eyelid, it may feel hard (even like a stone at times). Compare this with a normal eye. More accurate assessment of the intraocular pressure can be made with an instrument called a Schiotz tonometer.
The patient needs urgent treatment including acetazolamide tablets and pilocarpine drops and must go to the hospital as quickly as possible. If the high pressure in the eye continues for even a few hours, the optic nerve can be damaged and the patient might lose all sight in the eye.
15. Trachoma

Do you know which eye disease is shown in these images?
It is trachoma. Trachoma is a disease that usually starts in early childhood and can result in blindness 20 or more years later. Trachoma is caused by an organism called Chlamydia Trachomatis. Complications are due to recurrent re-infection of the eye. Over a number of years this infection and inflammation leads to severe damage of the upper eyelid causing eyelashes to turn in and these rub on the cornea causing scarring and blindness.
You may have seen children with running noses, discharging eyes and many flies. Flies may carry the organisms that can cause this most common of all eye infections. About 500 million people are suffering from trachoma, and 6 million people are blind.
Poor hygiene and sanitation are recognised as major factors encouraging this infection. Daily washing of the face helps to prevent infection of the eyes by Chlamydia Trachomatis. The following four pictures show stages in the development of trachoma.
16. Trachoma

The picture of an everted eyelid (top left) has a conjunctival surface which is not smooth, but shows a number of small raised dots – these are follicles. There must be 5 or more follicles, each at least 0.5 mm diameter, to describe this picture as follicular trachoma. You may see this in children under 10 years of age. The eyes are irritable and watering. Often patients complain of a feeling of sand in the eye. Vision at this stage is not affected.
If a patient is infected only once, it is unlikely that there will be serious long-term effects. If, however, the patient is reinfected many times, perhaps because other children in the family have trachoma, the inflammation will get worse.
A more advanced stage of trachoma is evident in the picture of the everted eyelid shown top right. Here the conjunctiva is swollen and you cannot see the normal blood vessels. This stage of trachoma is called intense inflammatory trachoma (where at least 50% of deep tarsal vessels cannot be seen because of trachomatous inflammation). At this stage the disease is very infectious and can easily be passed on to others.
If a patient has had many periods of infection with trachoma, scarring of the eyelid will develop. This is also best seen in the earlier stages by everting the eyelid (bottom left). Fine or coarse streaks of scar tissue may be observed and this stage is described as trachomatous scarring. With the upper eyelid in its ‘normal’ position you may see one or a few lashes rubbing on the eyeball. This is trachomatous trichiasis (bottom right).
If the scarring becomes severe the eyelid turns inward and the eyelashes will rub on the eyeball. This is called entropion which was shown in the previous section. Eyelashes rubbing on the eye cause damage to the surface of the cornea. The patient complains of pain and discomfort in the eye. If this situation continues, the cornea develops ulceration and scarring and becomes opaque. Vision will be severely reduced.
An operation to correct entropion will relieve discomfort and pain and stop further loss of vision.
Patients with trachoma should be given tetracycline 1% eye ointment once a day for 4 to 6 weeks. In areas where there are mass distribution programmes, the oral antibiotic azithromycin is given.
Always advise these patients and their relatives about the importance of daily face washing and good hygiene. Also ask other members of the family to come for examination and possible treatment of their eyes.
17. Allergy and the eye
A very common and troublesome eye condition, usually affecting children, is vernal kerato-conjunctivitis. This is an allergic problem which is worse in the spring and summer. The patient complains of severe itching, the eyes are red and there are mucus strands. It is also called vernal or spring catarrh.
On the left is pictured typical vernal kerato-conjunctivitis in the region of the limbus (corneo-scleral margin).
The picture on the right shows an everted eyelid with pronounced papillae (or ‘cobblestones’) – characteristic of the condition. Fluorescein dye shows an associated corneal ulcer and in some cases a corneal plaque may form with reduction of vision.
Apart from simple symptomatic measures (such as warm compresses), anti-allergy and anti-inflammatory eye drops may be required.
NEVER use steroid drops or ointment without strict medical supervision.
18. Pterygium
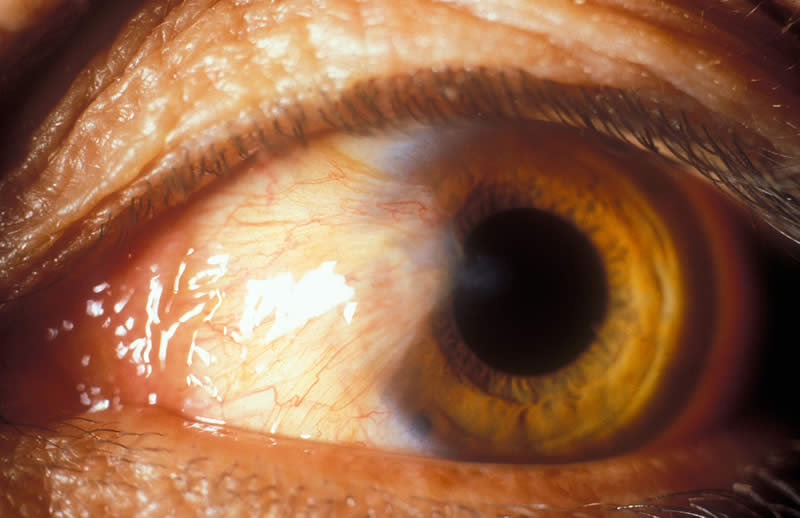
What is the fleshy growth shown in this picture? How would you manage this problem?
There is a wing of tissue at the nasal corner of the eye which is growing over the cornea. It is a pterygium. Surgery may be required to remove a pterygium. However, nothing should be done unless the pterygium grows to the centre of the cornea and is in danger of affecting vision. Surgery is often followed by a recurrence. Refer the patient for specialist advice it the pterygium is causing problems – either due to its size and position or if there is recurrent inflammation.
19. Corneal scarring

Scarring of the cornea usually has a grey-white appearance. The amount of scarring varies from a small scar which is peripheral on the cornea and does not affect vision to a very large scar where the cornea is completely white and opaque, with vision severely reduced.
Two examples of corneal scarring are shown in these pictures. Both scars involve the central cornea and vision is, therefore, affected.
Is there any treatment for these eyes?
The cornea shown on the left has clear cornea around the scar and would be suitable for an optical iridectomy or perhaps a corneal graft operation. An optical iridectomy is a surgical procedure where the pupil is enlarged so that the patient can see past the scar. If possible, the pupil is enlarged at the inferior and nasal part of the iris. A corneal graft requires a donor cornea and a specialist centre with the equipment and skills for this type of surgery.
The corneal scar shown on the right is almost a total corneal scar. Sadly, these eyes can seldom be helped. But if in any doubt, and if there is any possibility of help, especially in a patient who has scarring affecting both eyes, refer to the eye specialist for advice.
Note: If an eye is scarred and is also smaller and shrunken compared with a normal eye (phthisis), there is no advantage in referring such a patient in the hope of restoring vision. You may refer, however, if the eye is painful or inflamed. The eye surgeon may consider removing an eye which is blind and painful and replace this with an artificial eye.
20. Cataract
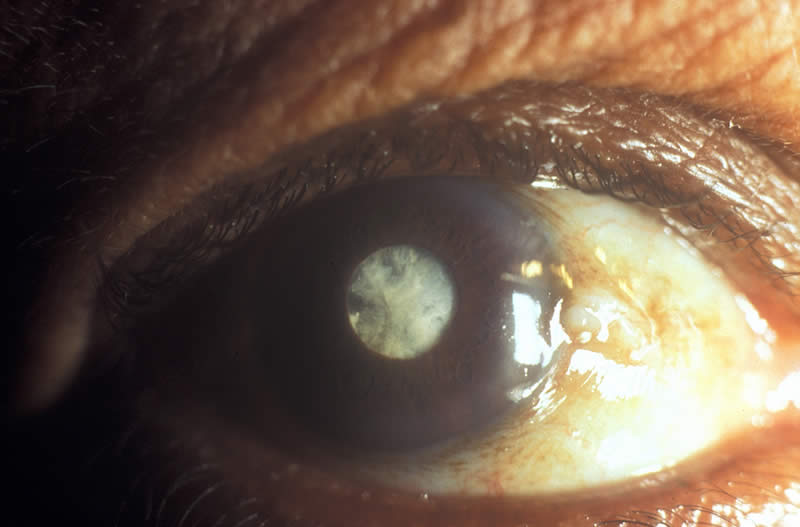
What is unusual about this eye?
The pupil does not look black; it is white. This is cataract. Approximately half of all cases of blindness in the world are caused by cataract. The lens has become cloudy. Usually both eyes are affected but it can occur in one eye only.
Most patients are elderly, but rarely children are born with cataract. The older patient will tell you that his vision has gradually become worse. He does not complain of pain. Ask your local eye surgeon when you should refer these patients. Certainly, if the patient is unable to count your fingers held at a distance of three metres, you should refer him for further examination and probable operation.
Blindness from cataract cannot be prevented, but it can easily be cured. The cloudy lens can be removed by surgery and replaced with an artificial lens. Following surgery, spectacles may still be needed for some patients to see better.
21. Strabismus
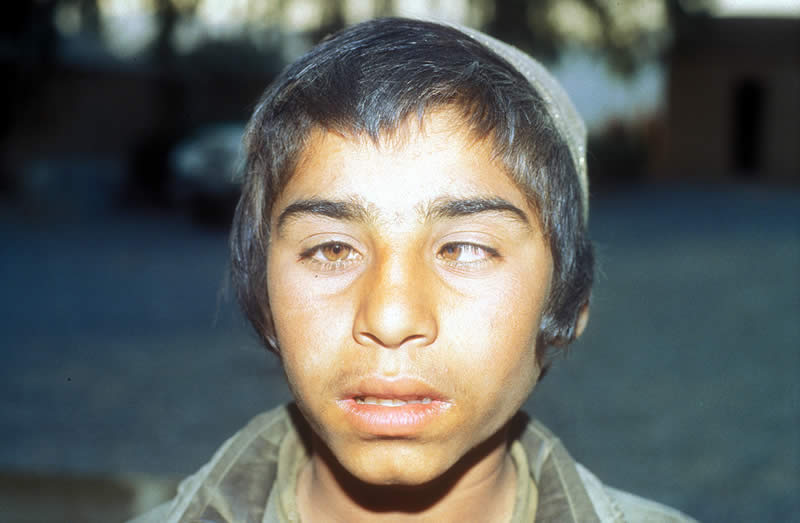
What is wrong with the eyes of this boy?
They are not straight. This patient has a marked squint, or strabismus. A squint may appear in a patient with apparently normal eyes. The older patient may have double vision.
If this happens in a child, the child often uses only one eye for clear vision. The other eye is not effectively used and becomes what is called a ‘lazy’ or amblyopic eye. If you treat such a patient in the first few years of life you can improve the vision in the lazy eye.
If an adult has had a squint since childhood, it is not possible to significantly improve sight in the lazy eye. When an adult develops a squint suddenly he may have double vision. This can be a sign of serious disease and the patient should be referred for further examination.
In any patient, if you see a squint or suspect a squint – refer for specialist opinion.
22. Refractive error

An eye problem which usually has a simple solution is the complaint of poor vision affecting eyes which look normal on first examination. The patient may describe poor vision for distant objects, where there is no problem with near vision – or it may be that the opposite is the case, distance vision is good but near vision has become poor. Also, vision can be poor for both distance and near.
The cause of poor distance or near vision may be a refractive error – the patient needs spectacles (or glasses).
A myopic, or short-sighted person, needs spectacles to see in the distance.
The patient who finds vision is blurred only for near vision is often middle aged and requires spectacles for close work. This is presbyopia. Patients over the age of 35 years who can see in the distance, but have problems reading, can often be helped by reading spectacles. The usual number needed is between +1.00 and +3.00.
A quick test to decide whether spectacles will or will not improve vision is the pin-hole test. Make a tiny opening in some cardboard or opaque plastic and ask the patient to look, one eye at a time, at an eye chart 6 metres distant. If looking through the tiny hole improves the visual acuity when compared with looking without the pin-hole, the patient should benefit from spectacles for distance vision. Refer to a colleague who can test for spectacles.
23. Leprosy

Two systemic diseases which may cause eye problems leading to blindness are leprosy and onchocerciasis (river blindness).
In this picture look at the face of the patient first, before you look at the eyes.
Which disease has been active here?
This is leprosy.
Although leprosy primarily affects the skin and nerves, the eyes are also very often involved. Always carefully examine the eyes of every leprosy patient even if there is no complaint about the eyes.
Look at the eyelids, check for ectropion (turning out) or entropion (turning in) and see if the eyelids move fully when the patient blinks. Ask the patient to keep the eyelids gently closed for 10 seconds. If it is not possible to close the eyelids, there is lagophthalmos. This leads to drying of the cornea and ulceration due to exposure. Remember that loss of sensation as a result of nerve damage in leprosy, means that these patients will often not complain of pain even if the eye has been damaged, for example, by a foreign body.
This patient has bilateral facial palsy, lagophthalmos, corneal exposure in the left eye, and corneal ulceration.
If a patient with leprosy has good vision in each eye, normal eyelids that can be kept closed, and round pupils that constrict with light, you do not have to refer to the hospital.
However, if the patient has a red eye, loss of vision, or inability to close his eye properly, refer for specialist advice.
Leprosy is an example of a systemic infectious disease where the eyes are often chronically affected but where an acute phase in the eye inflammation may also occur.
24. Onchocerciasis

Blindness is a severe disability. The picture on the left shows severe corneal scarring, in this case caused by onchocerciasis (river blindness). The old man, pictured on the right, is blind due to onchocerciasis and needs the guidance of a child.
To summarise some of the main points discussed, please note the following:-
1. At least half of all blind people can be helped to see again by cataract surgery. Recognise cataract (section 20) and refer these patients to a specialist.
2. Another 30% of blindness can be prevented or helped by:
- prevention and early treatment of ophthalmia neonatorum (section 7)
- prevention and early treatment of vitamin A deficiency (section 10)
- prevention and early treatment of trachoma (sections 15 and 16)
- early diagnosis and treatment of corneal ulceration (sections 11 and 12)
- prevention and early treatment of injuries (sections 3, 4, 5 and 6)
- correction with spectacles (section 22)
Learn to recognise eye conditions that can be cured.
Encourage programmes designed to prevent the onset of blindness.
For many people it is already too late to restore their vision and each blind person needs encouragement within the community, training in suitable skills and a belief that their lives can still be productive and fulfilling.
Their blindness should be a lesson for us all to do what we can to prevent blindness in future generations.
Acknowledgements
This teaching slide set was prepared by students of the ICEH Class of 1988 – Mr Jotham Bamuhiiga, Mr Mukti Gharti, Mr Trevor Graves, Mr Sidney Katala, Dr Hans Limburg, Dr Aroop Midya, Dr Balaravi Pillai, Dr Maria Rodrigues, Mr Thanaruk Suwanprapisa and Dr Shu-Tai Zhang – with Dr Murray McGavin. Later refinements were suggested by Professor Gordon Johnson and Dr Allen Foster. Secretarial assistance was given by Ms Faith Wakeford.
Photographs and artwork used in this teaching set are gratefully acknowledged:
- Dr Jock Anderson – Slides 5, 6a, 7, 9, 11a, 11b, 13, 14, 23
- Dr Allen Foster – Slides 3, 4a, 4b, 10a, 10b, 1 2, 1 6a, 1 6b, 1 6c, 1 6d, 24b
- Dr Hans Limburg – Slides 1 5a, 1 5b
- Dr Murray McGavin – Slides 1 a, 1b, 6b, 1 8, 20, 21, 22b
- Dr Gawn McIlwaine – Slide 8
- Dr John Sandford-Smith – Slides 1 7a, 1 7b
- Slidemotion Ltd – Slide 22a
- Professor Jan Stilma – Slide 24a
- Dr Richard Wormald – Slide 19b
- Ms Claire Wright – Slide 2
- Dr David Yorston – Slide 19a
Supported by CBM International, HelpAge International, Sight Savers International.
© 1992, updated 1995. International Centre for Eye Health, London School of Hygiene & Tropical Medicine, Keppel Street, London WC1E 7HT, United Kingdom