")
Trachoma teaching set. Full text
1. Trachoma
Major causes of blindness worldwide (in millions)
- Cataract 17.7
- Glaucoma 4.6
- AMD * 3.2
- Corneal opacities 1.9
- Diabetic retinopathy 1.8
- Childhood blindness 1.4
- Trachoma 1.3
- Onchocerciasis 0.3
- Others 4.8
* AMD – Age-related macular degeneration
What is trachoma? How many people are affected by trachoma?
Trachoma is one of the major blinding diseases of the world. It is the most common infectious cause of blindness.
Trachoma is caused by a recurrent, chronic eye infection. The organism involved is Chlamydia Trachomatis. Episodes of infection usually begin in childhood, while blindness from corneal scarring occurs after repeated infection, scarring of the eyelids, distortion of the eyelashes, associated trauma and secondary bacterial infection.
The World Health Organization estimates that 84 million people suffer from active trachoma and most of these are under 15 years of age. Up to 1.3 million are thought to be blind due to the eye disease.
The widespread distribution of trachoma throughout the world and the dangers of consequent blindness makes this eye disease a serious public health problem in many parts of Africa, the Middle East, Central Asia, India and South-east Asia. Trachoma is also found in some focal areas of Latin America and the Pacific region.
It should be noted that with improved living conditions and standards of hygiene in some countries, for example in Europe and Taiwan, trachoma has largely been eradicated.
Trachoma is a major cause of blindness worldwide. The list of eye diseases shown indicates the main blinding diseases as cataract, glaucoma, age-related macular degeneration, corneal opacities, diabetic retinopathy, childhood blindness, trachoma and onchocerciasis. In some severely affected areas, trachoma can be the most common cause of blindness.
2. Chlamydia Trachomatis

Trachoma is caused by the organism Chlamydia Trachomatis. Chlamydia Trachomatis is a highly infectious agent which can easily be transmitted from eye to eye. Using the microscope, a Giemsa stain of a conjunctival smear highlights the typical chlamydial inclusions, shown in the picture on the right.
The organism, Chlamydia Trachomatis, can pass from one child’s eyes to the eyes of other children within a few minutes, when they are playing together.
Chlamydia Trachomatis has been sub-divided into a number of serotypes, and the serotypes commonly associated with eye-to-eye infection are serotypes A, B or C.
The blinding effects of severe trachoma are a consequence of recurrent eye infection by the organism, often associated with seasonal purulent conjunctivitis. Repeated, untreated inflammation leads to scarring of the eyelids and corneas which results in visual impairment and blindness.
Note: Another pattern of transmission of Chlamydia Trachomatis is by sexual transmission. The serotypes of Chlamydia Trachomatis are different to the ones typically found in eye-to-eye infection. However, sexually transmitted Chlamydia Trachomatis, one of the venereal diseases, may also cause secondary eye infection and this is particularly important when the newborn child is found to have an eye infection which has occurred in the mother’s birth canal. This is one cause of ophthalmia neonatorum (newborn conjunctivitis). All newborn babies should have immediate application of tetracycline 1% eye ointment in each eye at birth, as a prophylactic measure.
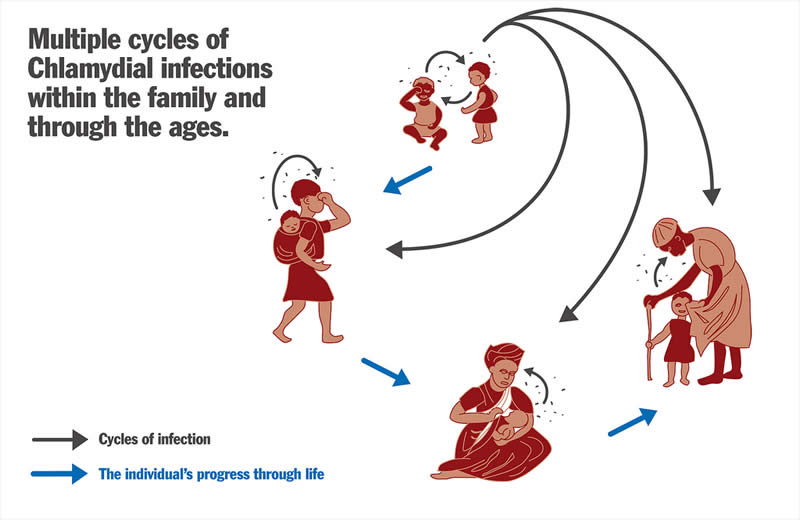
3. Risk factors for trachoma (1)

An environment which lacks effective sanitation, and adequate fresh water supplies, encourages transmission of the infection. Another environmental factor associated with transmission is the presence of animals kept near to dwellings and piles of animal dung provide breeding places for flies. Flies are attracted to red eyes with discharge, and carry the organism Chlamydia Trachomatis to the eyes of others within a family or a community, both children and adults. A further environmental factor associated with transmission is overcrowding in homes. This results in greater transmission amongst family members.
A cycle of re-infection within these populations needs to be broken by treatment, health education and preventive measures.
4. Risk factors for trachoma (2)

Which personal and community factors influence the transmission of trachoma and also the severity of complications of trachoma?
The picture shows an ‘eye-seeking’ fly attracted to the purulent discharge from an infected eye. The discharge from the eyes of an infected child may contain the infective organism which can be transmitted (carried) to the eyes of another child by flies.
Which conditions will attract flies?
Eyes which have discharge will attract flies. Nasal discharge attracts flies. Unwashed fingers may also transmit the organism.
Cloths or towels which are in contact with the face or eyes of a child may carry Chlamydia Trachomatis. Those caring for children often use a cloth or the edge of a piece of clothing to wipe away discharge from the eyes of an infected child. If the same piece of material is used to wipe the face of another child the infection will be transmitted. The family shown, top right, was described by the examining ophthalmologist as a ‘trachoma family’.
The presence of exposed faeces, whether human or animal, will attract flies and flies carry the organism Chlamydia Trachomatis. If there are suitable latrines in the community, these can certainly improve the situation, although the latrine must be properly designed and used. It is better if cattle can be kept at some distance from the family home.
Rubbish lying in open places attracts flies (bottom right).
One method to help our memories lists the six D’s:-
- Dry
- Dusty
- Dirty
- Dung
- Discharge
- Density (overcrowding in the home)
We can also summarise the factors which influence transmission of infection by listing the five F’s:-
- Flies
- Faeces
- Faces
- Fingers
- Fomites (contaminated material or objects such as clothing or towels).
A family home or surroundings which has many flies increases the risk of transmission of infection with Chlamydia Trachomatis. It is important to reduce the fly population in the community.
Flies can be kept to a minimum by:
- providing good sanitation, in the form of ventilated pit latrines (picture 22), or other types of latrines which are acceptable to the community
- burying or burning rubbish or collecting it at a site away from housing
- keeping animals at a distance from communities.
5. Risk factors for trachoma (3)

A dry, dusty area with exposed dung and poor sanitation is likely to have endemic trachoma.
The time taken to collect water from the primary water source is significant in affecting the prevalence rate of trachoma within a community. That is, the longer it takes to walk and transport water to the family home, the greater the possibility of trachoma within that home.
Clearly, available water increases the likelihood of good sanitation and good personal hygiene. Very little water is required to wash a child’s face and hands. The ‘leaky tin’ has been developed as a useful way of conserving water (picture 21). Provision of a good water supply may be an important intervention reducing the prevalence of trachoma in a community.
It is very important to improve both personal hygiene within families and also environmental sanitation. This advice, given to both young and old, will considerably influence the transmission of infection and so reduce acute and chronic inflammation, which over 10 to 20 years can cause scarring of the eyelids and corneas, with consequent blindness.
Does the provision of education have any effect on the rate of infection with trachoma in a community?
Lack of education, including health education, is associated with an increased risk of trachoma in communities. This is especially recognised in relation to inadequate education amongst mothers.
Economically poor communities are at greater risk of trachoma as their lifestyle is characterised by a deprived social status.
6. Age and trachoma
Are all age groups affected by trachoma?
All age groups may be affected by trachoma but there is a progression of the disease which may continue over many years, beginning in the very young, with the later scarring complications evident in older children and in all ages of adult life.
Children a few months old may be infected with Chlamydia Trachomatis, and in most heavily affected communities children aged 1 or 2 years will have the eye disease. In its early stages, trachoma may be very infectious, and the cycle of re-infection particularly involving children and mothers, needs to be broken to reduce the possibility of later complications.
It should be noted that Chlamydia Trachomatis has also been isolated from the upper respiratory and gastro-intestinal tracts in children.
7. Anatomy of trachoma
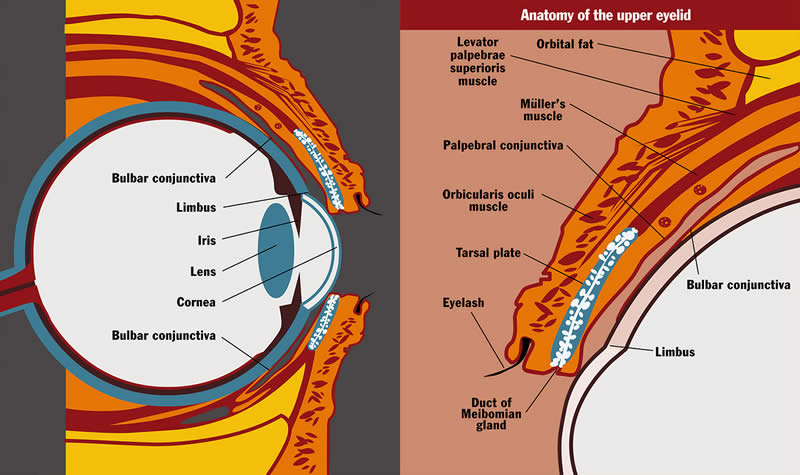
Before we discuss examination of the eyes for evidence of trachoma, we should consider the anatomy of the eyelid, conjunctiva, corneo-scleral margin (limbus) and cornea. We shall describe the function of the eyelids and their protective mechanism in association with the tear film.
What is the anatomy of the eyelids, conjunctiva, limbus and cornea?
The eyelids have four main layers of tissue – skin, muscle, tarsal plate and conjunctiva. The skin and muscle are closely bound together, as are the tarsal plate and conjunctiva, but the muscle layer and tarsal plate are only loosely connected and can be easily separated during surgery. Thus, from the surgical point of view, the lids consist of two layers – skin/muscle and tarsus/conjunctiva. The tarsal plate is attached by its upper border to the main elevator muscle of the eyelid by a thin layer of smooth muscle called the palpebral or Müller’s muscle. The conjunctiva above the upper border of the tarsal plate lies on this palpebral muscle up to the fold of the fornix where it is reflected down over the globe of the eye.
Between the loosely connected surgical layers, the main nerves and blood vessels lie, and their branches pass above the tarsal plate to reach the conjunctival membrane under which branches pass upwards and downwards. Here they can easily be seen when the eyelid is everted.
The conjunctiva lines the back of both upper and lower eyelids (palpebral conjunctiva), turns back on itself in the upper and lower fornices and continues over the surface of the eyeball (bulbar conjunctiva) to reach the corneo-scleral margin (limbus).
The corneo-scleral margin will often develop characteristic inflammatory changes of trachoma, particularly at the upper aspect, where it is exposed to the inflammatory changes of the upper palpebral (tarsal) conjunctiva. This area of upper corneal inflammatory haze is called pannus.
If the corneal epithelium is damaged, healing can take place without any residual scarring. Any damage which is deep to the corneal epithelium will usually result in scarring. The cornea has the following layers from front to back – corneal epithelium, Bowman’s membrane, the stroma, Descemet’s membrane and the corneal endothelium.
Abnormalities affecting the following makes the cornea vulnerable to infection:-
1. The corneal epithelium.
2. The tear film.
3. The eyelid.
What are the functions of the eyelids and the tear film?
The eyelids are beautifully designed to fulfil their main function which is to protect the eye. They mould perfectly over the contour of the cornea. Their movement in blinking ensures that the tear film is swept evenly and regularly across the surface of the cornea.
The strong sphincter muscle (orbicularis oculi) strengthens the eyelid’s protective mechanism against outside injury. Eyelashes act both as sensors to initiate a blink reflex and as barriers to insects and other foreign bodies.
A vertical row of Meibomian glands is contained in each tarsal plate – the eyelid ‘skeleton’. The ducts of these glands open onto the eyelid margins to release an oily fluid which helps to contain the tear film, reducing its evaporation and inhibiting its overflow onto the cheeks.
8. Clinical examination for trachoma

How should we examine each eye for signs of trachoma?
Examination of each eye should ideally be carried out with at least x 2.5 magnification, either using a single loupe or a binocular loupe (bottom left).
It is important to have good light, and a bright torch (flashlight) should be available if the examination is performed indoors. Sunlight may be adequate if the examination is made in the open with the patient facing the sun. As the patient is asked to look down in order to evert the upper eyelid, this procedure is acceptable for the patient.
If it is possible, both the patient and the examiner should be seated facing one another.
If the patient is a small child it may be necessary to restrain the child who will probably be distressed by the examination. A sheet or blanket is wrapped around the arms and legs of the child. An assistant can hold the arms and legs. The seated examiner controls the child’s head, gently, but firmly, between the knees. Alternatively, another assistant may hold the head. Both the examiner’s hands are free. Examination of the eyes can proceed.
After an initial assessment of each eye for conjunctival inflammation or the presence of any discharge, the eyelids should be carefully examined to see if any eyelashes are turned inwards and rubbing against the cornea (trichiasis). Evidence of removal of any eyelash or eyelashes (epilation) should be noted. The cornea is then examined for evidence of corneal opacity.
Following examination for evidence of eyelashes turning in, or corneal opacity, the upper eyelid is turned over (everted). After explaining that the examination is not painful, ask the patient to look down, but keep the eyes open. A glass rod, or other suitable narrow rod, is held parallel to the eyelid margin against the upper eyelid skin, just above the upper border of the tarsal plate. The eyelashes are grasped gently with the other hand and the upper eyelid is folded upwards. The upper tarsal conjunctiva will then be visible (bottom right). The appearance of the normal upper tarsal conjunctiva is pink and has a smooth surface. The conjunctival blood vessels will be clearly seen.
There are 5 clinical signs described in the grading of trachoma and these will be discussed with pictures 9-15.
9. Clinical presentation of trachoma
Trachoma: grading system
TF = Trachomatous inflammation – (follicles): five or more follicles, at least 0.5mm in size, on the ‘flat’ surface of the upper tarsal conjunctiva.
TI = Trachomatous inflammation – (intense): inflammatory thickening of the upper tarsal conjunctiva with more than half of the normal deep tarsal vessels obscured.
TS = Trachomatous scarring: scarring of the tarsal conjunctiva (fibrosis).
TT = Trachomatous trichiasis: at least one eyelash rubbing on the eyeball or evidence of eyelash removal.
CO = Corneal opacity: where at least part of the pupil is blurred or obscured.
How may a patient with trachoma first present with the disease?
The clinical picture of trachoma may vary from a very mild eye disease, with minimal symptoms and signs, to severe, chronic inflammation leading to blinding cicatricial eyelid deformities and corneal scarring. The patient can be a child with mildly irritable and red eyes, although often the condition is apparently asymptomatic. There may be associated discharge which usually indicates secondary bacterial infection. More severe, active disease will present with obviously red eyes, eyelid and conjunctival oedema, irritation, sometimes pain and photophobia. Blurring of vision may be associated with a muco-purulent discharge present on the cornea or involvement of the corneal epithelium in the disease process.
Long-standing trachoma with eyelid scarring causes trichiasis, where eyelashes are turned inwards and rub on the cornea and bulbar conjunctiva. Entropion and trichiasis, together with corneal scarring, are usually found in adults and more commonly in women. However, older children may also show features of the later scarring complications.
Trichiasis is often associated with entropion, where the eyelid margin, distorted due to scarring, is turned inwards against the eyeball. In trachoma this typically affects the upper eyelid.
In 1987, the World Health Organization published a simplified system for the assessment of trachoma and its complications. This is useful for diagnosing trachoma in a particular individual as well as assessing the magnitude and severity of the problem in communities. The system can also be used to monitor the results of medical treatment and of other control strategies.
The WHO system for assessment of trachoma is as follows:
- TF = Trachomatous Inflammation – Follicular
- TI = Trachomatous Inflammation – Intense
- TS = Trachomatous Scarring
- TT = Trachomatous Trichiasis
- CO = Corneal Opacity
This simple grading system describes the progression of eye disease, and its severity, but does not include all features of the disease process.
10. Inflammatory trachoma – follicles (TF)
TF = Trachomatous Inflammation – Follicular: the presence of 5 or more follicles, each of which must be at least 0.5mm in diameter, on the flat surface of the upper tarsal conjunctiva.
How would you describe trachomatous follicles?
The picture shows a number of follicles in early, active trachoma. These are tiny accumulations of lymphoid cells. The follicles are rounded, slightly raised and usually paler than the remaining conjunctival surface. It should be noted that the follicles must be on the flat surface of the tarsal conjunctiva which overlies the tarsal plate. The corners of the everted eyelid and the lower edge of the everted conjunctiva should not be considered in confirming this grade of trachoma.
11. Inflammatory trachoma – intense (TI)
TI = Trachomatous inflammation – intense: marked inflammatory thickening of the upper tarsal conjunctiva that obscures more than half of the deep conjunctival vessels.
The clinical presentation of trachoma now shows increased inflammation and is recognised as being a highly infectious stage of the disease process.
How would you describe the tarsal conjunctiva in the picture shown?
The infection is at a very active stage. The tarsal conjunctiva is thickened and inflamed. There is diffuse inflammatory infiltration with oedema and enlarged vascular papillae. For this grade to be described, more than half of the deep conjunctival vessels must be covered with inflamed conjunctiva so that the blood vessels are no longer visible. In the picture, the deep conjunctival vessels are not seen. It will be noted that trachomatous follicles are also present. Note that there is not yet any evidence of conjunctival scarring.
12. Conjunctival scarring of trachoma (TS)

TS = Trachomatous scarring: the presence of scarring in the tarsal conjunctiva.
How would you describe the appearance of fibrous scarring of the tarsal conjunctiva shown in the picture?
The white/yellow lines form a ‘basketwork’ of fibrous scarring in the tarsal conjunctiva. Scars may appear as white lines. They may also appear as bands or sheets which may take a variety of shapes and angles, sometimes looking like the edge of a feather.
Scarring is usually seen in adults but may occasionally be present in older children.
Notice that the tarsal conjunctiva is not so thickened although the deep conjunctival vessels are not clearly seen.
Trachomatous scarring may progress to cause distortion of the upper eyelid which results in the appearance of trachoma described in the following picture.
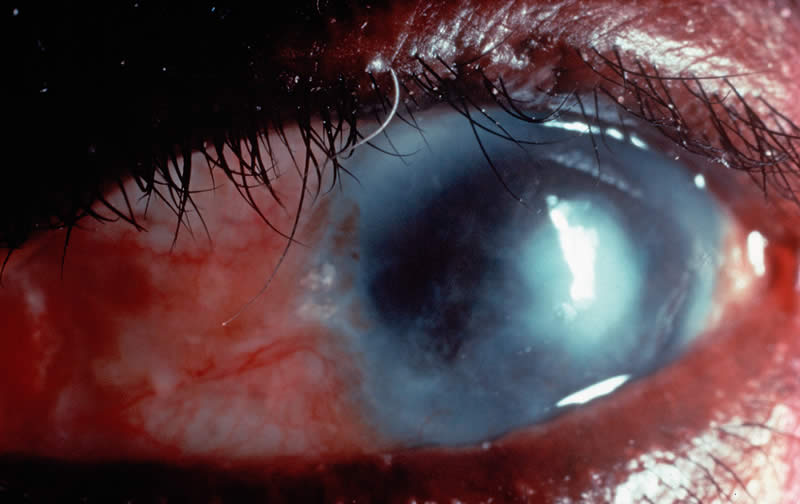
13. Trichiasis of trachoma (TT)
TT = Trachomatous trichiasis: evidence of one or more eyelashes rubbing on the eyeball. If one eyelash or a number of eyelashes have recently been removed, then the patient’s trachoma should be graded as trachomatous trichiasis also.
Trichiasis is more common in women than men and usually starts in adolescence, increasing in prevalence with age.
Some patients with trachomatous trichiasis will regularly remove eyelashes which have caused irritation by rubbing on the cornea. Usually this is done using a small pair of forceps and the patient may carry a small mirror or some other polished surface to use when removing the troublesome eyelash (picture 18). The removal of the eyelash in this way is called epilation. An eyelash will grow again in about 4 to 6 weeks. The procedure may then have to be repeated.
If eyelashes are rubbing on the cornea due to advanced conjunctival scarring and distortion of the upper eyelid, then a surgical procedure is necessary to relieve the situation. Surgery for an upper eyelid that is turning in (entropion) will be discussed with picture 19.
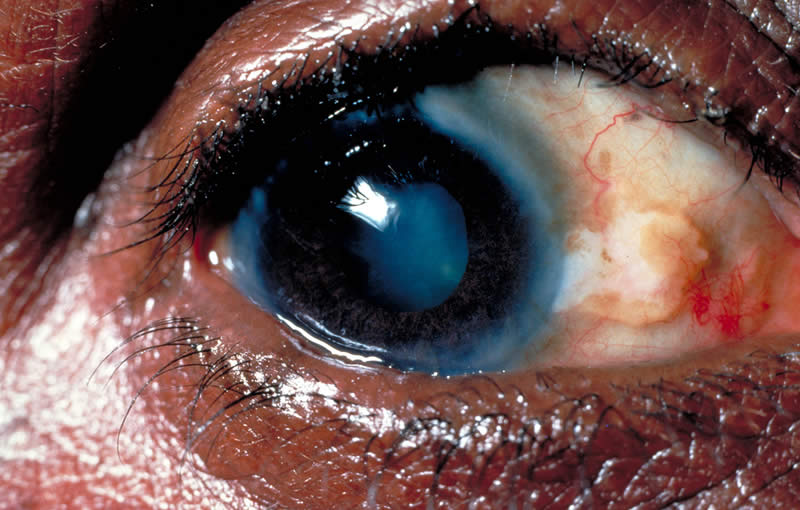
14. Corneal opacity due to trachoma (CO)
CO = Corneal Opacity: corneal scarring due to trachoma where the scarring is central and sufficiently dense to obscure part of the pupil margin.
Does the picture show an eye with ‘end stage’ corneal scarring due to trachoma?
This patient has significantly reduced vision due to corneal scarring. The eye still has some evidence of conjunctival inflammation. An eye ointment should be given but the patient must be advised not to expect improvement in vision following medical treatment. Notice that there is trichiasis and surgery will be required to correct the position of the irritating eyelashes.
Corneal opacity due to trachoma is usually seen after the age of 20 years. We have considered the simple grading system of trachoma, which is based on the presence or absence of 5 selected ‘key’ signs. The next picture gives a summary of the assessment of trachoma using these 5 signs.
15. Summary of trachoma grading system

Can you place each of these pictures in the correct category?
Top left: eyelashes are turned in towards the eyeball and are rubbing on the cornea. This is one of the very irritating and painful stages of trachoma with constant scratching on the sensitive cornea. This is trachomatous trichiasis (TT); a potentially blinding situation.
Top centre: the cornea has become scarred and the corneal opacity covers the pupil. This is within the definition for corneal opacity (CO). Vision is seriously impaired.
Top right: a normal, healthy eye, without inflammation, where the eyelid has been everted. The everted eyelid shows the upper tarsal conjunctiva which is smooth and pink without evidence of follicles or inflammation. Also, the deep conjunctival blood vessels can be seen. When the eyelid is in its normal position the eyelashes will point away from the eyeball. The cornea will be bright and clear. The pupil and the iris will be seen clearly through the cornea.
Bottom left: the eyelid has been everted. There are a number of tiny follicles, typical of follicular trachoma, and these are situated on the flat surface of the tarsal (palpebral) conjunctiva. This is active trachoma – trachomatous inflammation – follicular (TF).
Bottom centre: the everted eyelid shows evidence of the highly infectious, increasingly active stage of trachoma. The conjunctiva is thickened and inflamed. There is oedema and the conjunctival surface is rough and irregular. In this patient papillae are clearly seen. The deep conjunctival vessels have been obscured. This is active trachoma – trachomatous inflammation – intense (TI).
Bottom right: the everted eyelid appears quieter than in the previous picture, but there is now evidence of scarring of the conjunctiva. This is trachomatous scarring (TS).
Note: the order of presentation of these pictures is the recommended order of clinical examination to identify the 5 signs of trachoma (excluding the normal eye shown top right).
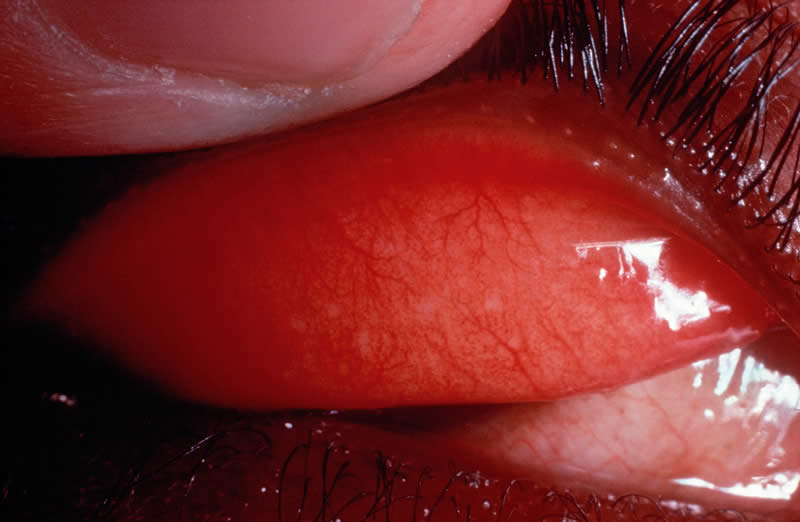
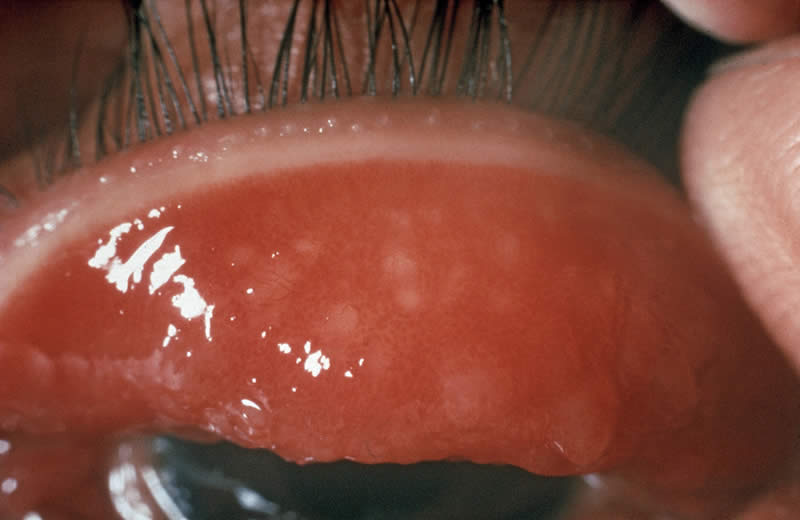
16. Differential diagnosis
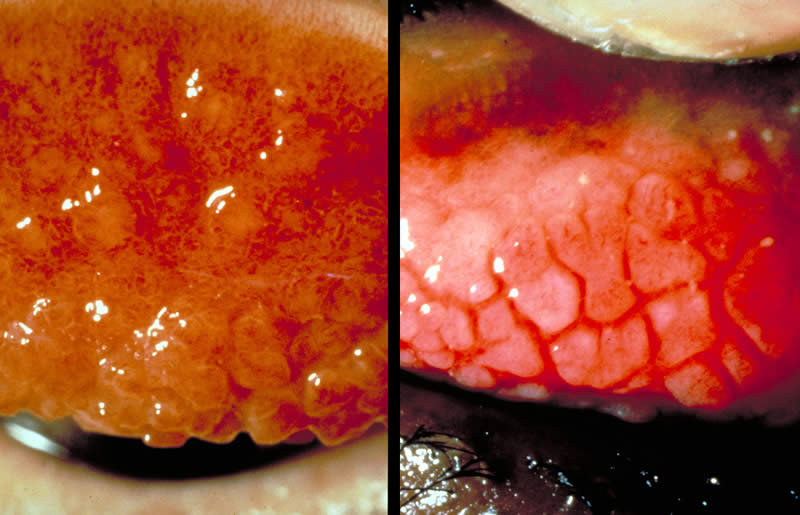
In making the diagnosis of trachoma, which other eye condition may be difficult to differentiate from trachoma and also may be present at the same time as trachoma?
An allergic condition affecting the eye may sometimes be difficult to differentiate from infection with Chlamydia Trachomatis. This condition is called vernal catarrh (also known as spring catarrh or allergic conjunctivitis). Vernal catarrh usually presents in children and is a chronic condition, particularly common in the spring and summer. It is characterised by itching, the eyes are red and irritable and there may be strands of mucus. In its florid state, typical papillae appear on the tarsal conjunctiva which often separate slightly from each other when the upper eyelid is everted. This appearance has been described as ‘cobblestones’, similar to the old street and road surfaces in many countries before tarmac surfaces were used.
In the pictures shown (left and right) which picture shows trachoma and which picture shows vernal catarrh?
On the left is shown a very intense inflammatory reaction of trachoma (TI) and, on the right, the typical papillae (cobblestones) of vernal catarrh. The similarities of the clinical appearances are obvious and, further, the two conditions may occur together in the same eye or eyes.
Active vernal catarrh may result in thickening of tissue at the corneo-scleral margin (limbus) and this characteristic appearance, if present, helps to differentiate trachoma from vernal catarrh.
The treatment of vernal catarrh is with anti-allergic or anti-inflammatory drugs which are not used in trachoma. We shall be dealing with the treatment of trachoma in the next four pictures. When in any doubt as to whether the condition is trachoma or vernal catarrh, treat first of all as trachoma and when the course of treatment for trachoma is well established or finished, review the situation and decide if treatment is required for an allergic condition also.
17.Medical treatment of trachoma
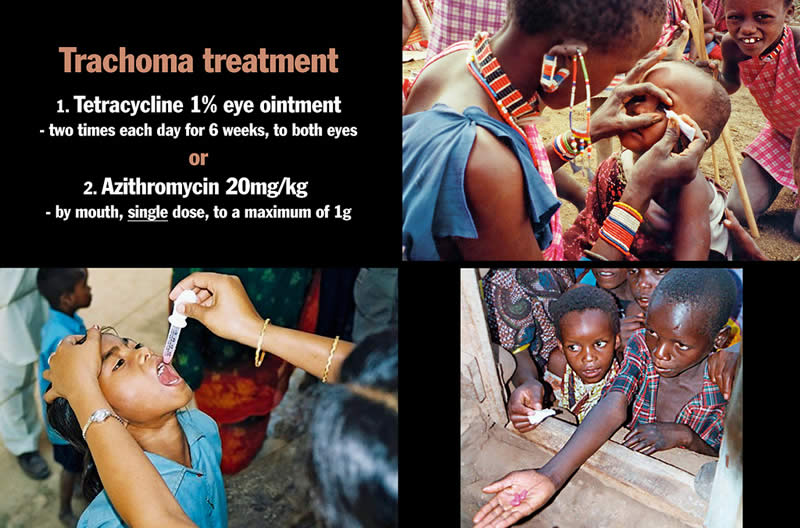
How should active trachoma be treated?
Treatment of active trachoma requires either
1. the application of tetracycline 1 % eye ointment to both eyes two times each day for 6 weeks, or
2. a single oral dose of 20mg azithromycin per kilogram of body weight, to a maximum of 1g. Azithromycin is available in both 250mg tablets and as a liquid suspension for small children or anyone unable to swallow tablets.
How should the ointment be applied?
If the child is old enough, or if the patient is an adult, he or she should be asked to look up. The lower eyelid is gently retracted from the eye and about one centimetre of ointment is placed in the lower conjunctival sac behind the lower eyelid (top right). The patient is asked to close the eye for about half a minute. The same procedure is carried out for the second eye.
Do antibiotics improve all grades of trachoma?
No – azithromycin or tetracycline ointment are effective only against active trachoma, particularly follicular trachoma (TF) and intense inflammatory trachoma (TI). It must be remembered, however, that active trachoma may be present in the eye which also shows scarring. It is advisable to give either azithromycin or tetracycline ointment whenever there is any possibility of active trachoma.
IMPORTANT
In some countries, it is recommended that azithromycin not be given to women during pregnancy or to children under the age of six months.
Adults with trichiasis and entropion, with or without corneal scarring, should be treated surgically. This will be discussed with slide 19.
Treatment for trachoma must always include reference to the need for good personal cleanliness, not only for prevention, but also as a vital part of patient care. Our purpose is to raise the standards of personal hygiene and care and so protect the eyes.
18. Trichiasis and epilation

How may a few eyelashes which rub on the eye be dealt with as a temporary measure?
We have seen that the scarring caused by trachoma affects the eyelids and also the clear ‘window’ of the eye, the cornea. Scarring of the eyelids causes the eyelashes to be distorted and these may constantly rub against the eyeball.
When only one or two eyelashes are causing trouble, a simple temporary measure is to remove each eyelash using forceps. The picture, bottom left, shows epilation forceps in use. A little mirror or polished surface may help in the removal of irritating eyelashes (picture on right). As eyelashes grow again in 4 to 6 weeks, the procedure has to be repeated when irritation recurs.
A more permanent method of dealing with an isolated ingrowing eyelash is to apply electrolysis, after injecting local anaesthetic into the eyelid at the base of the eyelash.
19. Surgery for upper eyelid entropion

How can we help the patient who has severe eyelid scarring causing the eyelid to turn inwards (entropion) with many eyelashes rubbing on the cornea?
This very uncomfortable situation requires eyelid surgery. There are a number of surgical procedures designed to rotate the eyelashes so that they are positioned away from the cornea. These procedures attempt to return the eyelid and eyelashes close to the original healthy situation, allowing the inside surface of the eyelid to move more evenly over the cornea.
The diagram shown top left indicates how scarring causes the eyelid to turn in so that eyelashes rub on the cornea. The recommended surgical technique, which is used to rotate the eyelashes and give considerable relief to the patient, is called bilamellar tarsal rotation.
A description of the bilamellar tarsal rotation procedure is published by the World Health Organization and the Edna McConnell Clark Foundation. The authors are Mark Reacher, Allen Foster, Janey Huber, with illustrations by Brent Bauer.
Can we improve vision after corneal scarring?
If the cornea is considerably scarred, then it is seldom possible to improve the eyesight. Corneal grafting is not usually successful in these eyes.
However, if there is an area of one cornea which does remains clear, where the scarring effects of trachoma involve the cornea in each eye, an optical iridectomy may be considered. In this surgical procedure, the pupil of the eye is made bigger so that the patient can look through the widened pupil which has been surgically enlarged behind the clear area of cornea. In this way, patients whose vision has been reduced to only hand movements, or counting fingers very close to the eyes, may be able to count fingers held at some metres from the eye. This can provide vision which allows the patient to walk more freely.
In some patients there can be slight improvement in vision after eyelid surgery for entropion and trichiasis – where there is some clearing of the corneal haze.
20. Prevention (1): personal and community hygiene
Trachoma: Community Hygiene and Sanitation
1. Good personal hygiene. Daily face washing/hand washing
2. A good water supply near to the community
3. Ventilated pit latrines
4. Animals housed at a distance from community homes
5. Health education
How does improved community hygiene and sanitation help to prevent trachoma?
Trachoma is often endemic in communities with poor social and educational opportunities and living conditions which lack adequate water and sanitary facilities.
The long term aim in the treatment of trachoma, within a community, must include raising individual and community standards of hygiene and sanitation.
1. Regular daily face-washing (and hand-washing).
2. The basic need of a suitable water supply near at hand.
3. Ventilated pit latrines to improve community hygiene.
4. Animals, especially cattle, housed, if possible, some distance from the family home.
5. Health education, arranged within the community – with community involvement in the planning and development of such a programme.
21. Prevention (2): face and hand washing

Why should face-washing and hand-washing be an important part of the prevention of trachoma?
The best method of dealing with trachoma is to prevent the infection which causes this eye disease.
The standards of personal hygiene and cleanliness for all age groups have great importance in avoiding many kinds of infection. This is particularly important in the prevention and treatment of trachoma.
Children must be encouraged to wash their faces regularly with water. Removal of discharge from the eyes and from the nose will reduce the likelihood of trachoma. This, in turn, will reduce the number of flies which are attracted to any discharge, and so the simple, regular act of washing the face (and hands) can break the cycle of re-infection with Chlamydia Trachomatis and secondary bacterial infection.
It is this cycle of re-infection which leads on to the scarring complications which cause unnecessary blindness. Trachoma as an eye-to-eye infection almost entirely disappeared in many countries simply because the standards of hygiene improved, and this was before the days when tetracycline was available!
How can very little water be effectively used to prevent trachoma?
Even if water is not freely available, it is surprising how little water can be used to prevent trachoma. It is important to pass on this message to mothers, children and all the community. The simple act of regular, daily hand and face-washing will prevent eye disease and even blindness (picture on left). The ‘leaky tin’ is one method of conserving water when the water supply is poor (picture on right). One litre of water can wash up to 30 faces.
A good water supply is of great value and importance to any community. Good water supplies will prevent many diseases which afflict millions of people around the world, and this is particular so in developing countries.
We should make sure that an effective primary water source is provided for each of the communities we serve.
22. Prevention (3): community health education: the environment
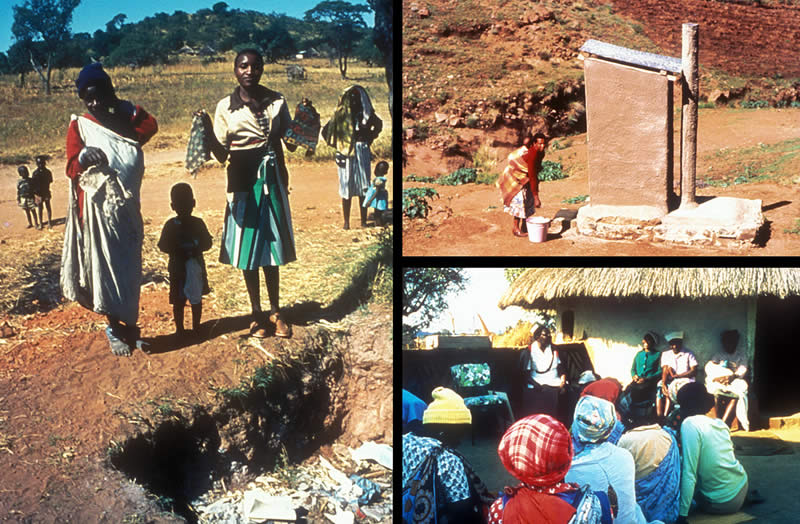
How can responsible members of the community prevent trachoma?
If school children are taught to wash their faces regularly, later there will be less infection with trachoma in their school community.
The picture on the left shows a small family group proudly demonstrating that each has an individual face cloth for face-washing. This responsible community has dug a refuse pit, which will reduce breeding places for flies.
Properly designed and used latrines provide a protective factor against trachoma. A well constructed, ventilated pit latrine prevents access to most flies and also prevents the escape of flies which do gain entry into the pit (top right). Human and animal faeces, which are exposed, attract flies which may carry the Chlamydial organism and an increased fly population in a community is associated with endemic trachoma.
Teaching should be provided for health workers, mothers, children and the community, advising them about red, irritable and discharging eyes when these appear in the family. Teaching should also be given about the prevention of eye disease in general (bottom right).
23. Public awareness and community participation: the SAFE Strategy

How would you advise a community about the prevention and treatment of trachoma?
Trachoma is an infective eye disease where public awareness and health education can be very important in controlling the disease.
Health workers should be sensitive to the effect their advice may have within communities, where changes in social and cultural habits may be suggested. A clear and honest message is required but with some understanding of the consequences to the lifestyles of individuals and communities.
Children in schools provide a captive audience ready to receive and accept new information. In one study in Africa the children were encouraged to wash their faces regularly. Soon children were encouraging each other in this good practice and the number of children with active trachoma was significantly reduced after six months.
Teachers have great influence in communities and should be taught themselves about the cause, risk factors, prevention and treatment of trachoma. Thus, both children and their teachers can change even lifetime habits and so improve personal and community standards of health care.
Instruction can be given about trachoma at other clinics, particularly mother and child health clinics.
In order to be effective and sustainable, the community needs to take part in trachoma control activities. With the assistance of members of the community, factors which encourage the spread of infection can be identified. Environmental and behavioural changes can therefore be brought about, with understanding and co-operation, in ways that are acceptable to the affected community.
What is the SAFE strategy?
The SAFE strategy emphasises to the health worker key points in the control of trachoma and the prevention of blindness.
S: Surgical correction of trichiasis (top left)
A: Antibiotic treatment of trachoma (top right)
F: Faces which are clean prevent the spread of diseases from child to child (bottom left)
E: Environmental changes (water and sanitation)
Surgical correction of trichiasis (picture 19) is often urgently required for patients who are at risk of becoming blind.
Antibiotic treatment of active trachoma (picture 17) is of particular importance where active disease (TF and TI) is diagnosed.
Facial cleanliness (picture 21) is a simple and effective method of preventing infection with trachoma and reducing the spread of disease.
Environmental improvements (picture 22) raise the standard of living of communities and give the opportunity of long term benefits by eliminating entirely this potentially blinding eye disease.
By the ordering of its letters, SAFE also emphasises the order of priorties in trachoma control. First of all, surgery to protect those at most immediate risk of blindness, then antibiotics for those at risk of blindness in 20 years time, then promotion of face-washing in a community setting and, finally, environmental improvements, which will require contributions
24. Trachoma control: assessment and strategy

We have studied trachoma, this widespread infectious eye disease which typically affects deprived populations, often living in poverty, unaware of basic health guidelines with poor personal hygiene, an unhealthy environment and an inadequate water supply. Dirty faces, hands and clothes attract flies which transmit the organism Chlamydia Trachomatis. Flies breed amongst refuse and rubbish, animal and human faeces, which may be found within and around such a disadvantaged community. Fingers and flies can quickly spread infection to the eyes, often affecting young children. A cycle of re-infection with superimposed secondary bacterial conjunctivitis results in a chronic inflammation which, in time, brings eyelid scarring, cicatrisation and distortion leading to corneal ulceration and opacity with consequent blindness.
In planning and implementing a programme for trachoma control the aims are:
1. To identify areas or communities where there is blinding trachoma, and/or severe active disease.
2. To provide eyelid surgery, antibiotics and health education to the communities at risk from trachoma.
How would you assess whether trachoma is a problem in the community?
One way is by a survey, which can give three important items of information about prevalence rates of the different stages of trachoma. The prevalence rate is a measure of the size of a problem at any one time.
1. The prevalence of active trachoma. This is the proportion of children in the community who at any one time have active disease (TF or TI). Active disease is most common in children under the age of 10 years, with the highest rates in pre-school and young children. Children with active disease and their families need antibiotic treatment.
2. The prevalence of TT. Trichiasis is most common in adult women. The prevalence of TT will give a guide as to how many people in the community need eyelid surgery.
3. The prevalence of CO. This will show how many people in the community are visually impaired or blind from trachoma.
Surveys are expensive to carry out and may not cover all the areas at high risk, so there is now research into a rapid assessment method for trachoma surveillance. This method uses a questionnaire to gather anecdotal and documented information about where the trachoma problem is likely to be most severe. The goals are:
1. Identification of areas or communities where there is blinding trachoma, and/or severe active disease.
2. A ranking of communities in order to prioritise the implementation of trachoma control programmes.
Who needs antibiotic treatment?
When the prevalence rates of trachoma are very high, almost every family will have most of the children affected and so the whole community will need treatment. As the prevalence rates fall it seems that trachoma clusters in families, so that in some families most children are affected while in others none are affected. This is most marked at very low prevalence rates where trachoma may persist in only one or two families in which most children are affected.
Antibiotic treatment is needed for all family members of any family in which there is an active case. It is not enough just to treat active cases without examining and treating the younger brothers and sisters at home. By leaving some family members untreated the cycle of re-infection will continue. A family member is taken to mean anyone who regularly shares a bedroom with the affected person.
A Strategy for implementing a trachoma control programme through the district health care system
(From the Report of the Second Meeting of the World Health Organization Alliance for the Global Elimination of Trachoma (GET 2020). WHO/PBL/GET/98.2. Reproduced by kind permission).
District programme model development
At national level
1. There is an urgent need to prevent blindness and visual impairment due to trachoma. This concerns, in the first instance, the timely treatment of trichiasis. It involves training of needed personnel, identification of cases, surgical treatment, and follow-up.
2. The other priority is to prevent potentially blinding trachoma (TF/TI). This involves the A, F, and E of the SAFE strategy. It requires the promotion of eye health by education to achieve behavioural and environmental changes.
The implementation of trachoma control is based on the following premises:
- It is modelled on SAFE
- It is an agreement with the public health framework, i.e., community-based, including monitoring and prevention as well as treatment
- It requires a national initiative
- It takes into account the fact that trachoma affects the most disadvantaged.
At the district level
- The magnitude and distribution of the problem is determined by rapid assessment
- The resource availability is determined
- This information is fed back to the national committee.
Surgical training
- Training in trichiasis surgery should be done at the district level
- A manual should be developed to cover all relevant training components
- The standard for adequate training could be short-term success (1-2 years) in 10 supervised eyelid surgeries.
Community-based personnel
The community ‘contract’ to work on trachoma allows volunteers to be elected. These volunteers are trained in case recognition and on how to mobilize the village; this activity is sustained by social recognition or payment in kind.
District co-ordinator
A district co-ordinator is required for:
1. Co-ordination of the A, F and E components.
2. Training of the community health workers.
3. Interfaces with the village leaders.
4. Providing data for programme monitoring.
The long-term aim
The objective in these strategies is to eliminate trachoma as a blinding disease. This initiative is called the WHO Global Alliance for the Elimination of Trachoma by the year 2020 (GET 2020). For eye care workers that motto has a very special meaning as 20/20 is perfect vision.
Acknowledgements
This teaching set was initiated by Dr Alberto Alberti, Dr Hago Babikir, Dr Felix Ezepue, Dr Arifa Gulab, Mr Ibrahim Liman, Dr Abdul Nabi, Dr Feyza Onder, Mr Georg Ort, Mr Bimal Poudyal, Mrs Gillian Sanosi, Mr Ansumana Sillah, Ms Susanna Simukonda, Mr Samuel Wilson, Mr James Yileyon, Dr Habib Yongolo, Dr Yolanda Zambujo, with Dr Murray McGavin, at the International Centre for Eye Health, Institute of Ophthalmology, London. Refinements were suggested by Professor Allen Foster, Ms Victoria Francis, Dr Clare Gilbert, Professor Gordon Johnson, Dr Denise Mabey, Dr SP Mariotti, Ms Susan Stevens and Dr Bjorn Thylefors. Information has been drawn from:
- Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organ. 2004;82:844-851
- Mariotti SP. New steps toward eliminating blinding trachoma. N Engl J Med. 2004;351:2004-2007
- WHO publication of the Second Meeting of the WHO Alliance for the Global Elimination of Trachoma (GET 2020)
Photographs and graphics in this teaching set are gratefully acknowledged:
- Anthony Solomon – Pictures 17b, 17c, 21a
- John DC Anderson – Pictures 1a, 2c, 4a, 4b, 10, 13, 14, 15d, 15f, 16a, 18a, 18b, 19c
- Mr H Anenden/WHO – Picture 23c
- Paul Courtright – Picture 3
- Filmstrip AV Services – Pictures 1b
- Allen Foster – Picture 11
- Victoria Francis – Pictures 17a, 21b
- John Hubley – Picture 22b
- Pak Sang Lee – Pictures 9, 20
- Tom Lietman – Pictures 8a, 8b, 8c, 8d
- Hans Limburg – Picture 24a
- Hugh Lugg – Pictures 7a, 7b, 19a
- Murray McGavin – Pictures 2a, 4d, 15a, 15c, 16b, 18c, 23a, 23b, 23d, 23e, 24d
- Mark Reacher – Picture 19b
- Erika Sutter – Pictures 5, 6, 17c, 22a, 22c, 24b, 24c
- Professor Hugh Taylor – Pictures 4c, 12, 15b, 15e
- John Treharne – Picture 2b
Supported by International Trachoma Initiative, CBM International, Sight Savers International.
© 1999, updated 2007 International Centre for Eye Health, London School of Hygiene & Tropical Medicine, Keppel Street, London WC1E 7HT, United Kingdom