")
Prevention of childhood blindness teaching set. Full text
1. Childhood blindness worldwide
How many children in the world are blind?
The exact number of children blind in the world is not known but it is estimated that the figure is approximately 1.4 million, with up to 500,000 new cases every year. Many of these children die within months after they become blind.
The frequency and causes of blindness vary widely in different parts of the world: in Africa and parts of Asia, up to 15/10,000 children are blind, compared to 3/10,000 children in Europe and North America; nutritional factors and infections are more common in developing countries, whereas hereditary factors, developmental disease and the consequences of prematurity are more frequent causes in countries with better standards of living and health care services.
Much of the eye disease which can cause blindness can be either prevented or treated. Our task as health workers is to preserve healthy eyes and avoid the situation of the boy shown in the picture who has corneal scarring of both eyes and is blind, with all of adult life ahead of him. Also, we can seek to influence policy makers, advising them how improved health care can prevent eye disease.
2. Causes of childhood blindness
What are the main causes of blindness in childhood?
Over a million children in Asia and Africa are blind and the single commonest avoidable cause is corneal scarring, due mainly to vitamin A deficiency. In Africa, corneal ulceration leading to corneal scarring is often associated with measles infection, and in Asia severe diarrhoea may lead to acute vitamin A deficiency causing blindness. Other causes of corneal scarring are conjunctivitis of the newborn (ophthalmia neonatorum), herpes simplex infection and the use of harmful (traditional) eye medicines. These causes are all preventable or treatable.
In many developing countries measles infection and vitamin A deficiency are being well controlled, and in these countries congenital and developmental cataracts are becoming relatively more important. Cataracts are a treatable cause of blindness in children.
In many middle income countries, particularly in Latin America and Eastern Europe, services for premature babies have expanded, and in many of these countries retinopathy of prematurity is the single commonest cause. This is a potentially preventable condition which can also be effectively treated.
In industrialised countries, inherited genetic factors causing cataract and retinal dystrophies are major causes of blindness in children, as are the consequences of premature birth. In industrialised countries the majority of children are blind from conditions which are not readily avoidable.
3. Onset of blindness
Factors from conception: hereditary
- Familial cataract, Retinal dystrophies, Retinoblastoma
Factors during pregnancy
- Rubella, Toxoplasmosis
Factors at the time of birth
- Retinopathy of prematurity, Newborn conjunctivitis
Factors during childhood
- Vitamin A deficiency, Measles, Eye infections, Traditional eye medicines, Injuries
When do these eye conditions affect a child?
For the purpose of this teaching set we recognise that a child is aged 0-15 years.
A simple classification divides the causes of childhood blindness into four groups depending on the time of onset of the condition leading to blindness:
1. Hereditary factors present from conception
2. Factors influencing the unborn child during pregnancy
3. Factors operating around the time of birth
4. Factors acting during childhood
5. Unknown
Hereditary factors which contribute to childhood blindness may cause, for example, familial cataract or retinal dystrophies. Damaging influences to the unborn child during pregnancy include maternal infection with rubella and toxoplasmosis. Examples of factors affecting sight around the time of birth are the effect of too much oxygen given to the premature baby (retinopathy of prematurity) and infection (newborn conjunctivitis). Blindness occurring in childhood includes conditions due to vitamin A deficiency, measles, external eye infections, harmful traditional eye medicines and eye injuries.
4. Examination for eye disease in children

A careful history should be taken, preferably from the mother who has had the closest contact with the child. Visual acuity should be assessed, and the findings recorded. Children over the age of 5 years can usually be tested with a Snellen E chart (top left), but children younger than this need to use other tests, such as pictures or matching methods. In very young children, a history from the parents and observation of the infant can help in determining whether the child is blind or not.
In some children, eye disease will be immediately obvious although this will not always be the case. The cause of the eye condition may be due to infection (top right) which in this child was beginning to improve with intensive topical antibiotics.
In the variety of eye problems which present at your clinic the picture may be more complicated and difficult to treat. The child whose eye is shown bottom left is a young boy, aged 5, who had trachoma. The infective, inflammatory condition, caused by the organism Chlamydia Trachomatis, had been made very much worse by treatment for two weeks with a harmful traditional medicine. The result was severe corneal scarring.
Some children will present with ‘quiet’ eyes but with considerable damage caused earlier in their lives. The boy pictured bottom right is blind due to dense corneal scarring, with distortion of the anterior parts of the eyes. A scarred, bulging anterior eye is called a staphyloma and is the result, in this case, of previous severe vitamin A deficiency. In children who are blind from conditions affecting their retina, optic nerve, or brain the front of the eyes appear entirely normal.
We shall now consider in more detail the common worldwide causes of blindness in children beginning with those leading to corneal scarring, all of which are preventable.
5. Vitamin A deficiency and the eye

Worldwide, vitamin A deficiency is the commonest single cause of blindness in children, accounting for an estimated 350,000 new cases each year. Vitamin A deficiency is also very important as it is associated with higher infant and childhood mortality rates, particularly associated with measles. It is estimated that 60% to 80% of children who become blind from vitamin A deficiency die within a few years because of increased susceptibility to infection and sometimes lack of care.
Recognition by health workers that vitamin A deficiency is causing blindness in children should also make them aware that children in these communities will be dying unnecessarily from a preventable cause. Health education for parents and communities is very important in preventing this nutritional disease.
Xerophthalmia is the term commonly used to describe an eye showing the clinical features of vitamin A deficiency. Literally, the term means ‘dry eye’ and one sign of xerophthalmia is the dry appearance of both the conjunctiva and the cornea, described as conjunctival and corneal xerosis. Vitamin A deficiency can also cause poor night vision due to lack of visual purple in the retina.
Vitamin A deficiency can occur for three major reasons:
- reduced intake of foods rich in vitamin A
- vitamins are not absorbed, usually because of diarrhoea
- increased need for vitamin A, as occurs during infections, particularly measles.
Blinding malnutrition is found in the developing countries of the world.
Which children are at risk of developing xerophthalmia?
While vitamin A deficiency can occur at any age, the group at risk of blindness is pre-school age children, from 6 months to 6 years of age.
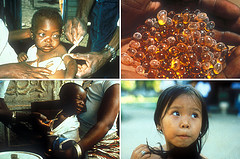
A typical child at risk of corneal blindness is a child who is one to 3 years old, no longer breast fed, who receives a poor diet and is malnourished, and who has developed measles (or another infection) or is suffering from diarrhoea. The child shown in the slide is malnourished and makes an unhappy picture – she is underweight, with obviously thin arms and legs. She has bilateral corneal ulceration due to vitamin A deficiency.
Measles is a particular risk factor in many countries and we shall look further at this important subject.
6. Symptoms and signs of xerophthalmia
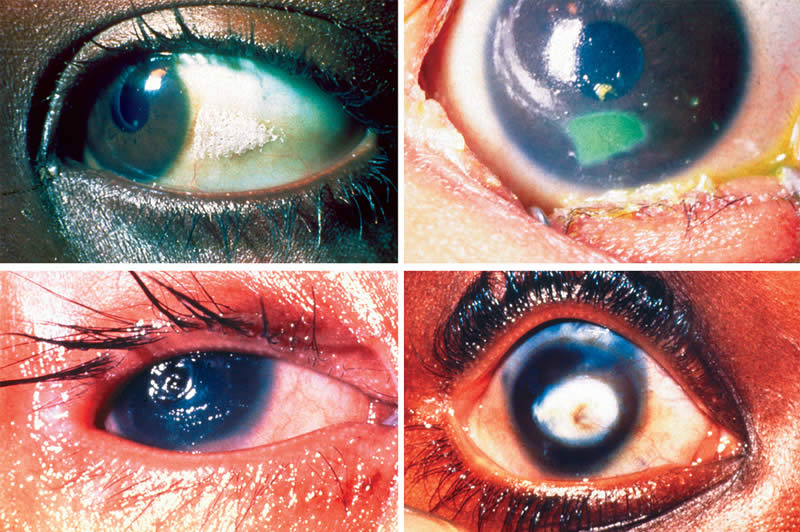
What are the symptoms and signs of vitamin A deficiency affecting the eye?
The following are the ocular symptoms and signs of vitamin A deficiency (xerophthalmia). The World Health Organization clinical codes are given in brackets.
Night blindness (XN): Vitamin A is needed to replace rhodopsin (visual purple) in the retina at the back of the eye and this is necessary for night vision. An adult or older child, on questioning, will describe the problem of night blindness but a very small child will not be able to offer this information. Ask the mother if the child cannot see as well as other children in the evening.
Conjunctival xerosis (XIA): Vitamin A is required for the production of secretions on the surface of the eye. This dry appearance together with xerosis of the corneal epithelium gives the condition its name, xerophthalmia. There is damage to the cells that produce secretions which moisten the surface of the eye.
Bitot’s spots (XIB): A Bitot’s spot has a typical white foamy appearance and is localised on the surface of the conjunctiva. Bitot’s spots may be found in both eyes, most often on the temporal conjunctiva. The picture shown top left is one example of a Bitot’s spot. These may appear in children under 3 years but are more common in older children. The appearance indicates changes in the squamous epithelium of the conjunctiva with underlying xerosis.
Corneal xerosis (X2): The surface of the cornea can have a typical dry appearance, and this can be seen in the picture shown top right. This eye also has an ulcer (see below).
Corneal ulceration with xerosis (X3A): The eye pictured top right has an inferior corneal ulcer which has been stained green with fluorescein dye. This area of ulceration places this eye in the category, corneal ulceration with xerosis (X3A).
Corneal ulceration/keratomalacia (X3B): This is the consequence of severe vitamin A deficiency. The onset is often sudden, and the cornea may melt very quickly, even over a few hours (keratomalacia). This development is most often seen in young children. The child shown bottom left has deep corneal ulceration progressing towards keratomalacia.
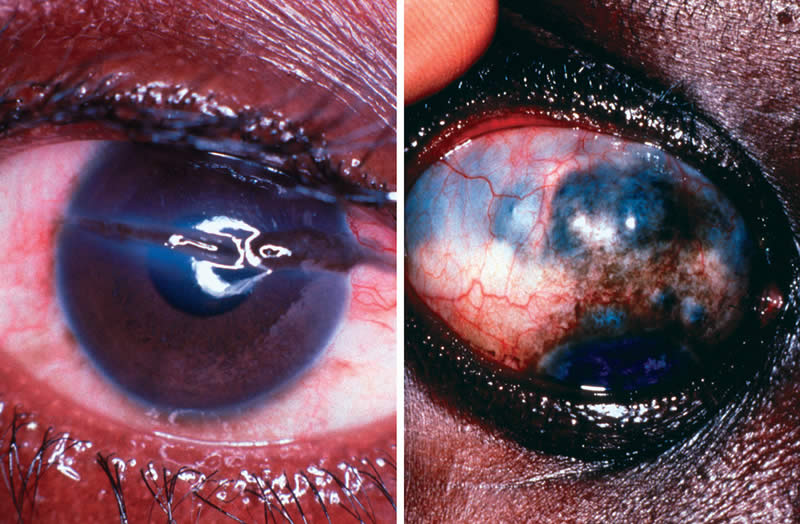
Corneal scarring (XS): The significant end stage of malnutrition causing eye damage, in a child who survives, is corneal scarring (bottom right). Corneal scarring often has a marked effect on vision. The anterior part of the eye may bulge forward (anterior staphyloma) or the opposite may occur and the eye shrinks (phthisis).
It is important to realise that not every child who is vitamin A deficient and at risk of blindness will have obvious eye signs. Finding evidence of xerophthalmia in one child will indicate that other children in the same family and community are also vitamin A deficient, even if they have no obvious signs. A child may have just enough vitamin A but have very little reserve in the liver. If a child becomes ill with measles, for example, vitamin A stores in the liver are rapidly used up resulting in acute deficiency. It is this situation that characteristically causes very rapid and severe corneal melting (keratomalacia) which results in blindness.
Learn to recognise the symptoms and signs of xerophthalmia. Not only will you save a child’s sight but you may also save a life.
7. Treatment of xerophthalmia
Children over one year
- Immediately on diagnosis (Day 1): 200,000 IU vitamin A orally†
- The following day (Day 2): 200,000 IU vitamin A orally
- Four weeks later (Week 4): 200,000 IU vitamin A orally
† If there is vomiting, an intramuscular injection of 100,000 IU of water soluble vitamin A (not an oil-based preparation) may be used instead of the first oral dose.
Children under one year old or < 8 kg
- Use half the doses of the regimen given above.
How would you treat a child with symptoms or signs of vitamin A deficiency?
The World Health Organization recommends the following treatment schedule for children over one year old who have xerophthalmia.
- Immediately on diagnosis (Day 1) – 200,000 IU vitamin A orally†
- The following day (Day 2) – 200,000 IU vitamin A orally
- Four weeks later (Week 4) – 200,000 IU vitamin A orally
† If there is vomiting, an intramuscular injection of 100,000 IU of water soluble vitamin A (not an oil-based preparation) may be used instead of the first oral dose.
If a child is under one year old or, at any age, weighs less than 8 kg: Use half the doses of the regimen given above.
- Immediately on diagnosis (Day 1) – 100,000 IU vitamin A orally
- The following day (Day 2) – 100,000 IU vitamin A orally
- Four weeks later (Week 4) – 100,000 IU vitamin A orally
The third dose of vitamin A in both regimens may be given between one and 4 weeks if follow-up is likely to be uncertain.
A topical antibiotic eye ointment such as tetracycline 1% or chloramphenicol 1%, 3 times a day, is recommended to reduce the possibility of secondary bacterial infection of the eyes.
Carefully apply an eye pad to the eye, making sure the eyelids are closed under the eye pad. Do not press on the eye – there is always the danger of perforation if corneal ulceration is present.
The child should be referred immediately to the eye specialist.
How would you treat a woman of reproductive age who is deficient in vitamin A?
Women of reproductive age should not receive large doses of vitamin A which are contra-indicated in pregnancy. If a woman has night blindness or Bitot’s spot she should have a daily dose of 10,000 IU of vitamin A orally for 2 weeks.
Immediately after the birth of her child a woman may be given 3 doses of vitamin A 200,000 IU, on Day 1, Day 2, and Day 8, to ensure a good supply of vitamin A in her breast milk for the newborn baby.
8. Prevention of xerophthalmia

How can we prevent xerophthalmia?
There are a number of approaches to the prevention of vitamin A deficiency in children.
1. Education in nutrition is required to encourage breast feeding. Colostrum and breast milk contain vitamin A. Weaning foods should be rich in vitamin A, for example, mango or papaya. Dark green leafy vegetables (DGLV) may be given at one year and older.
It is important that the mother herself has an adequate intake of vitamin A.
Give advice regarding which foods have a high content of vitamin A – for example, spinach, carrots, sweet potatoes and red palm oil (used in West Africa). Vitamin A is stored in the liver, and both animal liver and fish liver oils are good sources of vitamin A.
Encourage the planting of small gardens with advice as to which fruits and vegetables should be grown. Examples are shown top right – mango, papaya, dark green leafy vegetables and carrots.
Overcooking and drying fruits in the sun both reduce the vitamin A content of foods.
2. Vitamin A capsules 200,000 IU may be given every 3 to 6 months to children aged 1 to 6 years of age who are at high risk – as a short term measure (bottom left). Half doses are given to children between 6 and 12 months or if a child weighs less than 8 kg.
Each child with measles infection should have at least one dose of vitamin A 200,000 IU orally even if his or her eyes appear healthy. If there is any evidence of eye involvement, or if the child is known to be at high risk of xerophthalmia, 3 doses should be given on Day 1, Day 2 and after 4 weeks.
A programme of measles immunisation should be planned and carried out. We shall be discussing measles in more detail with the next section.
Immediately after her child is born a mother may be given 3 doses of 200,000 IU vitamin A orally on Day 1, Day 2, and Day 8 after delivery. This will help protect the breast-fed infant.
3. Foods may be fortified with vitamin A, for example, by fortifying a widely used food such as sugar. In the picture (bottom right) these refugee children are collecting milk which has been prepared from powdered milk fortified with vitamin A and vitamin D.
Remember the importance of public knowledge of the eye condition. Posters may be placed in hospitals, schools and other meeting places. Women and schoolgirls (the mothers of the next generation) especially need education. Teach other health workers. Use radio programmes, if available.
School children provide a ‘captive’ audience. Why not arrange a school drawing competition on the subject of eye health? Ask a well known person to come and give prizes to the winners of the competition.
9. Measles and corneal ulceration
Measles is a serious condition, not only because it can cause blindness, but also because it is an important cause of mortality. Both blindness and the death of a child can be prevented by recognising the condition quickly and treating the child with high doses of vitamin A.
How does the measles virus affect the eye?
If a child has measles there is usually photophobia, watering, red eyes, and closer examination may show a superficial punctate keratitis. A few children with measles develop true corneal ulceration and in half of these children both eyes are affected. It has been found that many children in blind schools have a history of measles infection before they become blind.
Why does measles cause eye problems?
1. The reserves of vitamin A may be low in the child and measles causes increased use of the remaining vitamin A. The sick child will have loss of appetite, often with gastro-enteritis. Intake of vitamin A will be reduced, together with the protein required for transport of vitamin A around the body. Thus, acute corneal ulceration and keratomalacia may rapidly occur and blindness result.
2. The fever associated with measles and depression of the activity of the immune system may allow secondary infection by the herpes simplex virus. We shall look at this complication in section 11.
3. Because the child’s eyes are inflamed and red, the mother may turn to a traditional healer and try a local remedy. These traditional eye medicines (TEM) can be harmful and make the condition worse and even cause blindness. We shall discuss TEM in section 12.
4. A corneal ulcer may develop in an ill and dehydrated child, who lies with his or her eyes open, which leads to drying of the exposed corneas. Always give a topical antibiotic eye ointment at least 4 times daily during the illness and avoid corneal exposure.
The diagram shown summarises the influence of measles in causing corneal blindness.
10. Prevention and treatment of measles

How can we prevent epidemics of measles?
The ill child shown on the left has measles – it can be prevented by immunisation. As measles is caused by an extremely infectious virus, immunisation programmes need high coverage to prevent epidemics (>80%). The Expanded Programme of Immunisation (EPI) of the World Health Organization is increasing the coverage of immunisation in children and many countries are achieving high coverage, but some, mainly in Africa, are not. Immunisation should be done at around 9 months of age, or soon after. Many programmes give 100,000 IU vitamin A at the time of immunisation, which is a good preventive measure.
How should we manage a child with measles?
1. Give vitamin A 200,000 IU orally at least once.
2. Supportive treatment of the child with measles is necessary to deal with any significant systemic involvement, for example, respiratory infection or gastroenteritis.
3. Instil a topical antibiotic into both eyes at least 4 times each day and avoid corneal exposure.
4. Children with measles should be given high dose vitamin A, which will help to preserve their sight and may save their life. The following regime should be used: For children over one year old:
Day 1: 200,000 IU vitamin A orally*
Day 2: 200,000 IU vitamin A orally
Week 4: 200,000 IU vitamin A orally
* If there is vomiting, give intramuscular water soluble vitamin A 100,000 IU instead of the first oral dose.
Children under one year or less than 8 kg weight should be given half doses of the above regimen.
5. Admission to hospital may be necessary. Many children are very ill with this disease.
11. Herpes simplex virus

How may the herpes simplex virus cause corneal blindness?
We have already referred to the danger of corneal ulceration due to the herpes simplex virus. Eye infection with the herpes simplex virus may be an increasing problem in developing countries and occurs in all age groups. The child pictured top left has measles and severe herpes simplex keratitis affecting the right eye.
The presentation of corneal ulceration in many regions may not have the classical appearance (dendritic ulcer) often seen in western countries. An example of the typical, branching dendritic figure, where the ulcer is stained with fluorescein dye, is shown top right.
The herpetic ulcer may be extensive, and is then described as a geographic or amoeboid ulcer. Examples are pictured bottom left, where the ulcer is stained with fluorescein dye, and bottom right, where deep ulceration and inflammation was evident in an eye which had been untreated for six months. Some of these ulcers have been given treatment with topical corticosteroids which has made the ulceration much worse. Steroid eye drops or ointments must not be used except by an expert – they can cause great harm when used at the wrong time.
We have seen that herpes simplex infection can complicate the corneal picture in measles. It is often found also in children with malaria or malnutrition, and in adults with HIV/AIDS.
A child or young person with corneal ulceration similar to those shown in the pictures should be referred immediately to the eye specialist. The specialist will give one of a number of topical antiviral preparations. The most commonly available is idoxuridine. Other more effective treatments are acyclovir and trifluorothymidine.
As with any corneal ulceration, healing may occur with scarring which can cause significant loss of vision.
12. Harmful traditional eye medicines

When are traditional eye medicines used?
Traditional eye medicines (TEM) are used for a great variety of eye diseases. The result of their use is often a more complicated clinical picture because the local remedy may cause further harm to an already abnormal eye. The TEM may be a “home remedy”, or may have been used at the suggestion of a traditional healer.
Measles is one example of a common infective condition causing a red eye where TEM may so worsen the clinical picture that corneal ulceration and blindness may follow. In deciding whether the appearance of a child’s eye or eyes has been influenced by TEM, the history is important. Keep in mind the fact that the mother may be very reluctant to admit that TEM has been used. She will realise that the community health worker will generally not approve the use of TEM.
How may traditional eye medicines affect the eye?
Traditional healers use a variety of substances in treating the eyes. They may use herbal medicines, the juice of squeezed plant leaves, lime juice, kerosene, toothpaste, breast milk and urine (either animal or human). Not all substances are harmful, but some may cause a chemical or caustic keratoconjunctivitis, others may introduce infection, such as bacterial infection with Neisseria Gonorrhoeae from human urine, or fungi from plant materials.
An unusual appearance of an eye which does not seem to have a typical clinical appearance, together with an accurate history, if this is given or admitted, will help make the diagnosis.
The little boy photographed top left has been treated with a red staining substance, which is made from ground down red rock (stone).
Traditional eye medicines have caused dramatic chemosis (inflammatory swelling of the conjunctiva) of each eye in the child shown top right. The picture bottom left shows a cornea which is thinned and Descemet’s membrane, the inner layer of the cornea, is bulging forward (Descemetocele) – there is a real danger of perforation. In the picture bottom right traditional eye medicines have contributed to the corneal scarring which may have been present before a traditional form of treatment was used.
Treatment is not easy and depends on the findings. Give topical medication with an antibiotic. A child with an eye condition made worse by TEM should be referred immediately to the eye specialist.
13. Newborn conjunctivitis
Which infectious condition involving a newborn child can cause blindness?
Conjunctivitis of the newborn (ophthalmia neonatorum) is a very serious problem in many parts of the developing world. Babies born to mothers with infection of the birth canal are those at risk (e.g. those with gonorrhoea, a sexually transmitted disease). The conditions starts as conjunctivitis, but sight can be lost if the infection involves the cornea. As the condition usually affects both eyes, the tragedy of an otherwise healthy child becoming blind must be avoided.
How do we recognise conjunctivitis of the newborn?
By definition, conjunctivitis of the newborn occurs in a child within the first 30 days of life. Two organisms commonly cause conjunctivitis of the newborn.
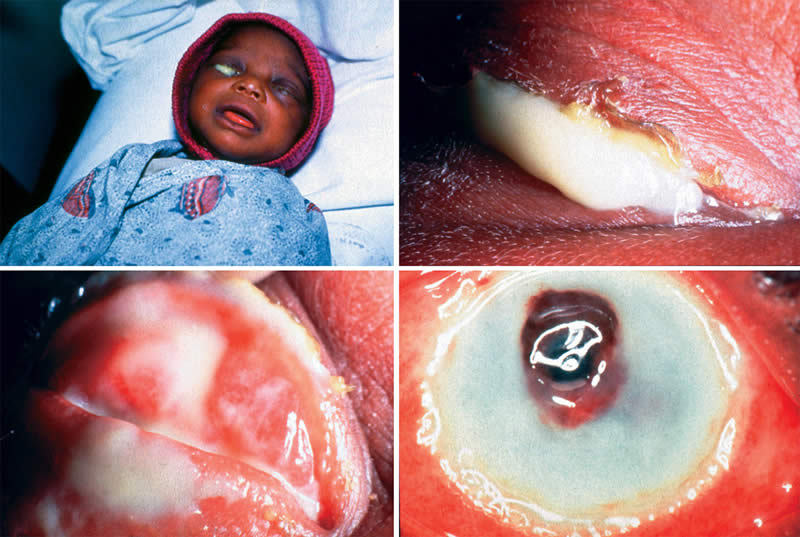
Neisseria Gonorrhoeae causes bilateral purulent conjunctivitis with considerable discharge which may accumulate behind tense and swollen eyelids. This condition usually presents in the early days of life and corneal involvement can progress to ulceration and perforation. Severe corneal scarring may cause blindness. The picture top left shows a newborn child with purulent gonococcal conjunctivitis affecting both eyes. A close-up view of one eye in the same child (top right) shows pus squeezing between tense eyelids. The picture bottom left reveals inflamed conjunctivae with purulent discharge. This is an eye emergency and treatment must begin immediately. Failure to prevent this condition or treat the infection quickly can result in the tragedy of the eye shown bottom right, where the cornea is severely infected and will later be grossly scarred. When examining a child with this infection be careful when opening the tense eyelids as pus may spurt into your own eye! However, it is necessary to examine the cornea and, also, to instil antibiotics so that they come into direct contact with the cornea and conjunctiva. Wash your hands thoroughly afterwards.
Chlamydia Trachomatis is the other organism which may commonly affect the eyes of a newborn child. In these children the infection has a less dramatic presentation, causing irritable, red eyes but without purulent discharge, unless secondary bacterial infection has complicated the picture.
Usually the infection presents later than gonococcal infection and some of these children may not be brought to the clinic.
The clinical picture of newborn conjunctivitis may be confused if a child is given traditional eye medicines (TEM) by a local healer.
Infection with these organisms is not confined only to the eyes but can involve the other systems of the body, so treatment requires systemic therapy as well as topical eye medication.
Other bacteria which may cause newborn conjunctivitis are Haemophilus, Streptococcus pneumoniae, Staphylococcus and Pseudomonas.
14. Treatment of newborn conjunctivitis
Neisseria Gonorrhoeae
- Penicillin IM or Cefotaxime 100mg/kg IM
or Kanamycin 25mg/kg IM - Tetracycline 1% or Erythromycin 0.5% eye ointment hourly on first day – then 3 hourly for 3 days, followed by 3 times daily for a total of 14 days
Chlamydia Trachomatis
- Erythromycin estolate syrup orally 50mg/kg each day for 14 days.
Systemic treatment of both parents
How would you prevent infection causing conjunctivitis of the newborn?
An effective procedure for preventing infection is prophylactic treatment of the newborn child. The procedure involves cleaning the eyelids, and the use of topical antibiotics or antiseptics. As soon as every child is born (preferably when the head is just delivered) the eyelids must be carefully cleaned with moistened, sterile cotton wool. A single application of tetracycline 1% eye ointment is then instilled into each eye. Silver nitrate 1% eye drops or povidone iodine 2.5% may also be used in each eye if tetracycline is not available. If used, silver nitrate must have been well preserved in a closed bottle, avoiding exposure to light. Each preparation should be used for a single dose and discarded after use.
Other methods of preventing conjunctivitis of the newborn include antenatal screening of pregnant women for gonococcal and chlamydial infections, with systemic antibiotic treatment of those found to be infected.
How would you treat conjunctivitis of the newborn?
When infection has been caused by Neisseria Gonorrhoeae the child should be admitted to hospital and intramuscular penicillin should be given. Topical medication is also applied to the eyes and tetracycline 1% eye ointment may be used, hourly on the first day, 3 hourly for 3 days, then reducing to 3 times daily for a total of 14 days. In some regions penicillin-resistant Neisseria Gonorrhoeae is found and alternative single injections are intramuscular cefotaxime 100 mg/kg, or kanamycin 25 mg/kg, together with 14 days of tetracycline 1% eye ointment. Erythromycin 0.5% eye ointment may be used instead of tetracycline eye ointment.
Systemic treatment for infection with Chlamydia Trachomatis should be given using erythromycin estolate orally, as a syrup, 50 mg/kg each day for 14 days. Systemic tetracycline should not be given as it damages developing teeth and bones.
An important part of treatment for these infections is systemic treatment of both parents as both may carry the organisms.
Infection with other organisms should be treated with tetracycline 1% eye ointment or erythromycin 0.5% eye ointment 4 times daily for 14 days.
15. Corneal ulceration

How would you examine and treat a child presenting with a corneal ulcer?
We have already discussed treatment of different types of corneal ulcers. But we should consider our general approach to examination and treatment of a child presenting with a corneal ulcer.
1. History. Ask the parents, and the child also if old enough, how and when the eye trouble began.
Is the vision affected?
(Check the visual acuity of each eye in the older child).
Is there a history of night blindness?
Did the ulcer develop spontaneously?
Did the ulcer follow injury, for example, scratching by the branch of a tree?
(Injury with plant material could suggest a fungal infection).
How is the general health of the child?
What did the child eat yesterday?
Is there a history of measles, diarrhoea or malaria?
Have traditional eye medicines been used?
2. Examination. Examine the child’s general appearance.
Is the child malnourished?
Does the child have measles?
Is there any evidence of respiratory infection or gastro-enteritis?
Examine the eyes carefully using a focal light and magnification. Note the appearance of the ulcer or ulcers and of any discharge.
Is the condition affecting one or both eyes?
One Eye
- herpes simplex keratitis
- eye injury
- bacterial infection (one or both eyes)
- fungal infection
Both Eyes
- conjunctivitis of the newborn
- xerophthalmia
- traditional eye medicines (one or both eyes)
- measles
3. Corneal ulceration in children
Is there dryness of the eyes – or Bitot’s spots?
Is there discharge of pus?
(This will indicate bacterial or fungal infection)
Is there pus in the anterior chamber of the eye (hypopyon)?
Is there watering only?
(This occurs with viral infection and after injury).
Is there a typical dendritic figure of herpes simplex keratitis or a possible herpetic geographic ulcer?
4. Prevention and treatment
1. Prophylactic vitamin A, 200,000 IU orally, should be given at least once to a child with any one of the following:
– malnutrition
– diarrhoea
– measles
2. If there is evidence of corneal ulceration, vitamin A 200,000 IU is given orally on the first day, second day and after 4 weeks. (An injection of water soluble vitamin A 100,000 IU may be given on the first day instead of the oral dose, if the child is vomiting). Half doses – vitamin A 100,000 IU – are given to children under one year of age or less than 8 kg in weight.
3. An antibiotic eye ointment, such as tetracycline 1% should be used at least 4 times each day.
4. Atropine 0.5% eye drops or ointment should be given once daily.
5. An eye pad is applied.
6. The general condition of the child must be assessed and treatment given for systemic infection, malnutrition or diarrhoea.
7. The child is referred for specialist opinion and treatment.
Intensive antibiotic drops or ointment and/or a sub-conjunctival antibiotic injection will probably be required for bacterial infections.
If an ulcer, which is not obviously herpetic, fails to improve within a few days of treatment with an antibiotic, then the specialist may consider using an antiviral agent such as idoxuridine or acyclovir.
Obvious herpetic ulcers require treatment with antivirals.
It is not possible clinically to be definite in making a differential diagnosis between a corneal ulcer due to bacterial infection or fungal infection. The specialist may take a sample of pus and place a smear on a glass slide, then apply Gram’s stain to determine whether the infection is bacterial or fungal.
In the examples given in the photographs, the picture top left shows a child with bilateral corneal ulceration due to vitamin A deficiency. The picture top right has an eye with purulent corneal ulceration and pus in the anterior chamber (hypopyon). The photograph bottom left is of an eye with a geographic ulcer due to herpes simplex virus. The eye shown bottom right, with corneal ulceration and an iris prolapse, has developed complications following the use of traditional eye medicine, and the eye is at risk of becoming blind. Early diagnosis and early referral to the specialist for prompt and expert treatment is needed.
16. Corneal scarring

Each of the conditions causing corneal ulceration in childhood may heal, but, unless the ulceration is superficial, healing will leave a corneal scar (leucoma). Depending on the severity and position of ulceration the effect on vision will vary considerably.
Is there any way in which vision can be improved when corneal scarring is present?
If the scarring is confined to the central cornea, with an area of clear cornea present peripherally, and if the child has sufficient vision to be able to accurately detect the direction of a light being shone into the eye, then surgery may be considered.
One method of improving sight in a blind patient with bilateral corneal scars, but with an area of clear cornea, is an optical iridectomy. Peripheral iris is removed surgically from behind an area of clear cornea. An example of an optical iridectomy is shown in the picture on the left. The optical iridectomy has enlarged the pupil infero-nasally so that light can enter the eye once again. It is encouraging to see a young person, blind in each eye due to corneal scarring, achieve improved vision after an optical iridectomy, with new freedom to walk around.
Surgery must only be considered when all signs of inflammation have gone.
A centrally placed corneal scar may be suitable for corneal grafting using a donor corneal graft. This surgical procedure requires a surgeon experienced in the technique, an available donor cornea, microsurgical instruments, suitable suture material, an operating microscope and long term follow-up after surgery. This surgery is not usually recommended for children as the visual outcomes are generally not very good.
Extensive disease of the anterior part of the eye can result in a blind eye, which has no perception of light. An example is shown in the picture on the right. Sometimes chronic pain is a problem which can be relieved by removing the eye. An artificial eye should be fitted for cosmetic purposes.
17. Congenital cataract

All the conditions dealt with so far cause loss of vision due to corneal scarring, and we have seen that many of them are preventable, or can be treated, to limit the amount of corneal damage.
The conditions that will be described in the following slides are usually not preventable, but it is important that they are recognised, as treatment given at the right time can help restore or maintain vision. These conditions include congenital cataract, glaucoma, retinoblastoma, retinopathy of prematurity and eye injuries.
What is congenital cataract and how does it affect sight?
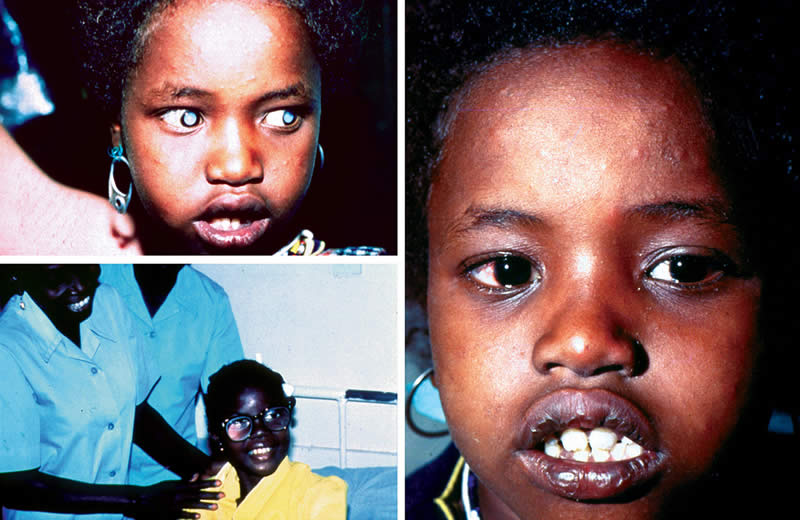
A cataract is an opacity of the lens of the eye. A child can be born with cataracts (congenital cataract), or the cataract can develop during childhood (developmental cataract). Look at the photograph of the child on the left. The centre of each eye, the pupil, is dark. This is the normal appearance. Now compare with the child on the right. The pupil area in each eye is densely white and opaque. These are cataracts and since both eyes are involved and the cataracts are dense, vision will be affected.
Cataract is the commonest cause of blindness in the world amongst adults. Cataracts in babies and children differ in two major respects from those in adults; firstly, in why they develop and, secondly, in how they are managed.
18. Causes and investigation of congenital cataract
What causes congenital cataract?
There are a number of different causes of cataract presenting in newborn children. Genetic factors we have mentioned previously, usually with “dominant inheritance” which means that the condition occurs in each generation. Since the condition is an inherited one, brothers and sisters may also be born with cataract. If there is a family history of cataracts, the parents need to be told of the risks of future children being affected, so that they can make the decision whether or not to have any more children.
We have also referred to infections affecting the mother in the early months of pregnancy, and some of these infections can result in her child having cataract. Rubella is the most common cause. Chickenpox and toxoplasmosis (infection with Toxoplasma gondii) in the mother may also cause cataract in the unborn child. Other causes include metabolic disorders, where certain substances, necessary for normal biochemical functions, are deficient. Down’s syndrome may be associated with congenital cataract.
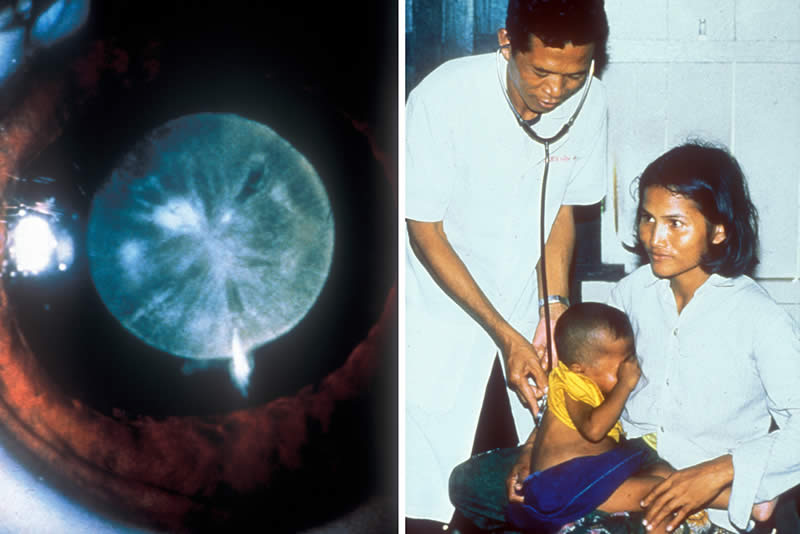
The mother of the child, whose congenital cataract is shown in the picture on the left, had rubella during the first 4 months of pregnancy. Notice that this cataract is dense and centrally placed. Children with the Congenital Rubella Syndrome may also have other congenital defects such as small eyes (microphthalmos), glaucoma, deafness, heart abnormalities, and defective growth and mental development.
How can congenital cataract be prevented?
Cataracts caused by congenital rubella can be prevented by immunisation. At present there are two different approaches; vaccination of all babies in infancy at the time of immunisation against measles (MMR – mumps, measles and rubella), and vaccination of young girls at puberty. The aim of both programmes is to prevent women from contracting rubella when they are pregnant, so preventing congenital cataract from this cause.
Careful consideration needs to be given before deciding whether rubella immunisation of infants, or of 12 year old girls should be introduced. To be safe and effective, coverage rates for infants (i.e., the proportion of infants in the community who are immunised) need to be very high. Immunising schoolgirls is not quite as effective, but is a safer strategy.
What is the approach to the care of a child with congenital cataract?
First of all, it is necessary to recognise cataract in a child. If you find a cataract in one or both eyes then refer the child for expert care.
1. Carefully examine the eyes of a newborn baby with a torch (flashlight). Make sure the pupil is round and reacts directly to light. Note the depth of the anterior chamber of the eye and the position of the opacity in the lens.
2. If cataract is present an accurate history should be taken from the parents.
Was the mother ill during the pregnancy?
Did she have a rash at any time?
Was this during the first 4 months of the pregnancy?
This might suggest a history of rubella.
3. The parents should be asked further questions.
Are there any other children in the family with the same appearance?
Do either of the parents have visual problems, or have they had eye surgery?
These questions are asked to determine any possible inherited abnormality.
4. Other features should be noted during a careful general examination (see picture on the right).
Is the baby otherwise healthy?
Is there any evidence of other congenital detects such as a small head, deafness or heart murmurs?
5. It will be wise to examine other children in the family and also the parents. Familial cataract may not have been noticed because vision has not apparently been affected.
6. Refer all children with a white pupil urgently for expert opinion. It is important that the diagnosis is confirmed as the differential diagnosis includes, for example, a life-threatening tumour in young children which also presents with a white pupil in one or both eyes. We shall discuss this tumour with section 21.
7. Thus, the following steps should be followed:
– Diagnosis of congenital cataract/white pupil
– History of the child’s general health, the mother’s pregnancy and the family
– Full eye examination
– General examination
– Urgent referral
8. Remember that the mother and father will be distressed that their new baby is not entirely healthy. Gently explain the reasons for your enquiries and that you want to provide the best possible care for the infant.
9. The treatment of congenital cataract is surgical.
10. After surgery long-term follow up is very important to ensure that there are no complications and that the child is seeing as clearly as possible.
19. Surgery for congenital cataract
How soon after birth should a child have surgery for congenital cataract?
The major difference in managing a child with cataracts, compared to adults, is that it is vital that the child is referred to an experienced ophthalmologist/eye surgeon for surgical treatment as soon as the diagnosis is made. This is because young children with dense cataracts will not develop vision properly as long as the cataracts are interfering with vision (top left). If surgery is delayed, this will result in a ‘lazy’ or amblyopic eye, which will not be able to see well. If surgery is performed quickly the vision will have a chance of developing satisfactorily.
If both eyes are affected the surgeon will operate on each eye with only a few days between the two operations. General anaesthesia will be required for younger children and so the decision regarding the time of operation must also consider the general health of the child.
Different surgical techniques are used to remove a congenital cataract. One method is to ‘suck out’ the cataractous lens material with special surgical equipment.
The child shown on the right is a 7-year old girl from Somalia who has just had surgery for congenital cataract. Ideally, surgery should have been carried out when she was younger. Remember to refer any child with a white pupil, or pupils, to the eye surgeon as soon as possible after this appearance is recognised.
If a clear pupil area is achieved after surgery, how is optical correction provided?
After surgery to remove cataract, light entering the eye is no longer in focus as the lens of the eye has been removed. In children it is very important that the light is focused again as quickly as possible so that normal vision can develop. (Aphakia is the situation where the lens has been removed from the eye).
Three methods are used to provide optical correction after congenital cataract surgery.
Intraocular lenses (IOLs) – these are small, plastic lenses which are inserted into the eye at the time of surgery. IOLs are now used routinely in adult cataract surgery, and are being increasingly used in children. For technical and optical reasons their use is not recommended for small babies.
Aphakic spectacles should be prescribed for the child who has had surgery for cataract where IOLs were not inserted at the time of surgery. A young child will often accept the spectacles quite well. The picture (bottom left) shows a child wearing aphakic spectacles.
It is necessary to carry out a refraction every 6 months and keep the child in the best spectacles possible. It is advisable to overcorrect distance refraction by one to 2 dioptres to encourage the use of near vision in the child. Often high plus dioptre lenses are needed in a small baby.
Contact lenses – these are difficult to fit, expensive and are often lost. (They may have a place in uniocular aphakia).
Whichever method is used the child will need to have long term follow up, to make sure the vision is as good as possible, which may mean changing their spectacles, or even performing another operation.
20. Congenital glaucoma

What is glaucoma?
Glaucoma is a condition which affects adults much more often than children. In glaucoma there is damage to the optic nerve of the eye, which leads to gradual loss of the peripheral field of vision and sometimes blindness. The damage is usually associated with an abnormally high pressure inside the eye.
Glaucoma in children differs from glaucoma in adults, as there are other ways in which the sight can be lost in addition to damage to the optic nerve. The glaucoma can either be present at birth, or it can develop during childhood. It can affect one or both eyes. The tissues of a child’s eyes are more elastic than an adult’s eye, and so they can stretch. This is what happens in childhood glaucoma. As the pressure inside the eye rises the tissues stretch, and the eye enlarges. This is why the condition is known as buphthalmos or ox eye.
Which symptoms and signs indicate childhood glaucoma?
The condition may be painful, and the child can be distressed. Loss of vision may be obvious. Light often makes the eyes more uncomfortable, and the child will try to avoid bright light (photophobia). The eyes may be watery, but there is no discharge or corneal ulceration. Careful examination of the cornea may show that it is larger than it should be, and the cornea may be cloudy. The pupil may react slowly.
The child will need an examination under anaesthetic, when raised intraocular pressure and cupping of the optic nerve head are typically found. The child in the picture has glaucoma affecting the left eye, which has become larger than the right eye. The cornea is hazy. In children, as in adults, glaucoma usually affects both eyes.
How should a child with glaucoma be treated?
In children, glaucoma surgery is the only effective treatment. This is different from adults where long-term use of eye drops can control the intraocular pressure.
After glaucoma surgery, long-term follow up is essential, to make sure the intraocular pressure is controlled and vision is developing as normally as possible.
21. Retinoblastoma

Which is the commonest malignant eye tumour in childhood?
Retinoblastoma is a malignant tumour which arises in retinal cells. Without treatment the tumour will almost certainly cause the death of the child. The most important factor in a child’s survival is early recognition of the tumour. If the tumour is advanced it will extend along the optic nerve to the brain and also break through the sclera after having filled a large volume of the vitreous cavity. In the later stages the tumour can spread to other parts of the body.
Look at the picture of the child on the left. At first sight the appearance is similar to the child with congenital cataracts. Closer examination of this child would reveal that the white reflex is caused by tumour tissue behind the lens of each eye. The picture on the right shows a more advanced tumour which has destroyed the eye; the tumour is filling the orbit and extending forward. When the tumour has extended outside the eye the prognosis for survival is much worse.
The tumour may present at any time during the first 5 years of life.
This malignant tumour of childhood may be hereditary due to abnormal genes in the parents. Other tumours occur sporadically. The tumour may be present in one eye or in both eyes. Retinoblastoma involving both eyes is usually hereditary in origin.
Presenting signs of the tumour within the eye may be a white appearance of the pupil (leucocoria) or a squint. Other presenting signs are glaucoma, poor vision, an abnormal pupil and orbital cellulitis. Sadly, many children are first seen with already advanced tumours, proptosis and an orbital mass.
How should a child with possible or definite retinoblastoma be treated?
The most significant influence on successful treatment is recognition of the tumour while it is still contained within the eye, followed by immediate referral to a specialist.
In most eye centres in developing countries the correct treatment is surgical removal of the eye (enucleation) taking as much of the attached optic nerve as possible.
Some centres have the facilities to provide radiotherapy and chemotherapy for these children, as well as the necessary surgical expertise. Early recognition and referral to an advanced specialist centre, which has the equipment and drugs available to give appropriate treatment, may allow up to 90% of children to survive.
22. Retinopathy of prematurity
What is retinopathy of prematurity?
Retinopathy of prematurity (ROP) is a potentially blinding disease which primarily affects preterm (less than 32 weeks gestation) and low birth weight (less than 1,500 gms at birth) babies. ROP was a major cause of blindness in children in Europe and North America in the 1940s and 1950s and is now becoming an important cause in Latin America, Eastern Europe and urban centres in Asia where it can also affect bigger, more mature babies.
Severe disease can affect up to 8% of premature babies.
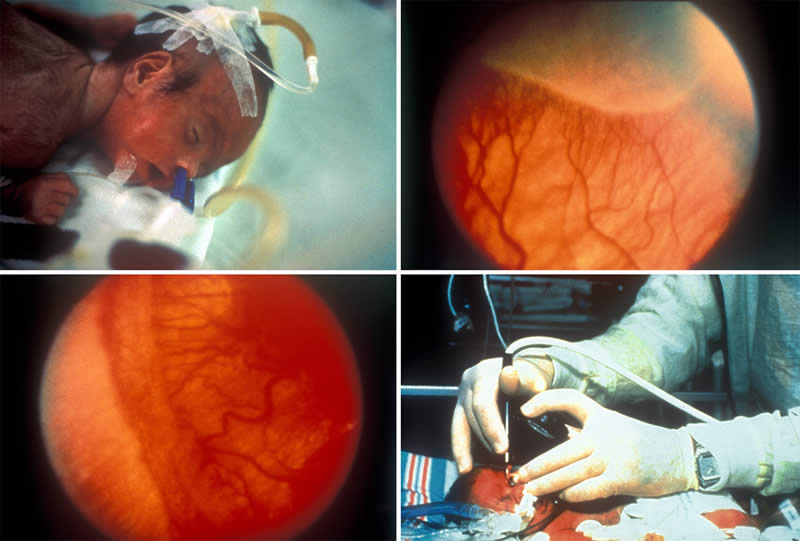
Retinopathy of prematurity occurs when the immature, developing retina is exposed to too much or fluctuating levels of oxygen, as occurs when unmonitored or poorly controlled supplemental oxygen is given to premature or low birth weight babies (top left).
The condition, which usually begins 6-7 weeks after birth, irrespective of how premature the baby, is characterised by the development of abnormal blood vessels at the boundary between vascularised, central retina and unvascularised, peripheral retina (Stages 1-3). Stage 1 disease is shown top right – with a clearly visible boundary between central, vascularised retina, and peripheral, avascular retina. This can progress to retinal detachment and blindness (Stages 4 and 5), but spontaneous regression also occurs in a high proportion of babies.
Prevention of blindness from ROP depends on preventing preterm birth (e.g., by good antenatal care of pregnant women, and reducing the rate of unnecessary Caesarean sections); very good intensive neonatal care of premature babies, with monitoring of blood gases, and early detection of the stage of ROP that needs treatment. Surgery to treat retinal detachment is complex, and often gives disappointing results.
How can a child with ROP be identified? What treatment is available?
To identify babies with ROP needing treatment, the first examination should be 6-7 weeks after birth. All babies weighing less than 1,800 gms, or born before 34 weeks gestation, should be included in the screening programme, which is probably best organised by the neonatologist or nurse in charge of the unit. The pupils need to be dilated with phenylephrine 1% and tropicamide 0.5%, and the retina examined by a trained ophthalmologist using an indirect ophthalmoscope, with scleral depression so that the retinal periphery can be adequately examined.
Eyes with Stage 3 disease (fibrovascular proliferation) with ‘plus’ disease (dilation of the retinal and iris blood vessels, with vitreous haze) should be treated straight away with either gentle cryotherapy or laser to the avascular, retinal periphery. The picture bottom left shows Stage 3 ‘plus’ disease with extensive fibrovascular proliferation (new vessels), and dilated, tortuous retinal blood vessels. A baby with Stage 3 ‘plus’ disease (bottom right) is being given gentle cryotherapy to the avascular retinal periphery under general anaesthetic.
The infants need to be followed up to ensure that the disease is regressing, and to see whether they are developing refractive errors, or strabismus, which are more common in premature babies.
23. Eye injuries
Injuries to the eye can be caused in many ways and by a variety of objects. Superficial injuries may heal without loss of sight. If a wound of the cornea is no deeper than the corneal epithelium healing will usually take place without scarring.
Which types of eye injury may be sight-threatening?
A general subdivision of ocular injury is:
1. Penetrating injury
2. Blunt injury
Penetrating injury. Injury with a sharp object, for example, a thorn, a knife, a needle, or a foreign body travelling at speed, may cause considerable damage to the eye. Damage in the line of the visual axis will have some effect on vision. Examples of injuries which may result in loss of vision are: a central laceration of the cornea, the development of traumatic cataract, haemorrhage into the vitreous and disturbance of the central retina. There is also the danger of infection being introduced into the eye by a penetrating injury. The picture on the left shows a horizontal laceration of the cornea with prolapse of iris through the wound.
Foreign bodies may be superficial (on the surface of the eye) or deep (in the cornea, or inside the eye). Superficial foreign bodies can often be removed under local anaesthesia, and then treated with antibiotic eye ointment. Deep foreign bodies, however, require referral to an eye specialist.
Blunt injury. The concussive effect of a blow on the eye, for example with a stone, a ball or a fist, is a common reason for a child to appear at the clinic. Damage may cause corneal oedema, haemorrhage into the anterior chamber of the eye (hyphaema), traumatic cataract and retinal oedema. In the picture on the right, previous injury to this eye has caused severe damage to the eye with areas of scleral thinning and bulging, showing the dark choroid beneath (scleral staphylomata).
In the case of acute injury to the eye, take an accurate history, record the vision in each eye, examine carefully and make exact notes. Give a topical antibiotic and then apply an eye pad making sure that the eyelids are closed under the eye pad. With a penetrating eye injury an eye shield should be placed over the eye, for example, a Cartella shield. If a commercially made shield is not available then old x-ray film, or card, cut and shaped to make a cone, can temporarily shield the eye and orbit.
An eye injury where vision is reduced requires referral to the eye specialist. Any uncertainty in diagnosis, or prognosis, should also mean referral of the patient for expert advice and treatment.
24. Summary
We have studied the important eye diseases that can result in blindness in childhood, placing emphasis on those that are preventable and/or treatable. We have also noted that the causes of childhood blindness vary considerably from country to country. To make an impact on the incidence of childhood blindness it is important to find out which are the major causes of blindness in your own country and community. In African and Asian countries the commonest causes are corneal scarring secondary to vitamin A deficiency, the use of harmful traditional eye medicines, conjunctivitis of the newborn and herpes simplex infection.
In Africa, measles infection can precipitate vitamin A related corneal ulceration, whereas in Asia this is often associated with diarrhoea. Cataracts are also important in Africa and Asia.
In Latin American countries, congenital cataract, whether of unknown cause, due to hereditary factors or maternal infection with rubella during pregnancy, and retinopathy of prematurity, are the more common causes.
In European countries and North America, the commoner causes are hereditary diseases, developmental abnormalities and retinopathy of prematurity.
The management of eye disease in children differs in several respects from that in adults. One factor is that the child cannot take responsibility for himself or herself, but is dependent on the decisions of adults, that is, the parents and yourself. In children it is much more important to act quickly if the child has a preventable or treatable disease. This is not only because a blind child may have a lifetime of blindness ahead, if treatment is delayed and therefore less effective, but, also, because the immature visual system of the child may result in a ‘lazy’ eye if treatment is not given early.
Many childhood conditions that result in blindness can be prevented, either by preventing the onset of disease, for example, by immunisation against measles; by prophylaxis to prevent conjunctivitis of the newborn, or by accurately recognising and treating important blinding conditions, for example, cataract.
The most important blinding childhood eye disease worldwide is vitamin A deficiency, which is why the recognition, treatment and prevention of this condition has been stressed in this teaching slide set. We conclude with photographs which emphasise this most significant blinding condition of childhood.
The child shown top left has corneal scarring. Measurement of the upper arm circumference is a very good method of assessing the nutritional status of a child aged between one and 6 years. Long term prevention of vitamin A deficiency requires education of communities on what to grow and what to eat. Measles immunisation (bottom left) will also help to prevent vitamin A deficiency within communities.
Around 1,500 children worldwide become blind every day. The little girl shown bottom right has eyes that are healthy and bright. We must seek to preserve healthy eyes and good eyesight in each of these young lives.
It is an important part of our work to share our knowledge of eye disease with other health workers and to inform people in the communities for whom we have responsibility, that childhood eye disease can often be prevented or cured.
Learn to recognise the eye diseases which can affect the eyes of children in your community and which may cause blindness. Begin treatment when you have the correct medicines available and feel secure in your diagnosis. If there is any uncertainty at all, or if follow-up is required, refer the child to the eye specialist for further care.
Even if we see a child that is incurably blind it is important to realise that this child needs our help too. Children who are blind have the same rights as children who can see, and they also need to play, have friends, experience different things and go to school. Most countries have educational programmes for children who are blind, either as an inclusive/integrated education programme, where blind children go to the same school as sighted children, or there may be provision in schools exclusively for children who are blind. Parents of blind children also need support and to be encouraged to let their child safely explore their environment so that they develop as widely and as fully as possible.
Acknowledgements
This teaching set on childhood blindness was initiated by Ms Luz Amparo Hernandez-Duran, Dr Sashyalatha Kotiankar and Dr Murray McGavin of the International Centre for Eye Health, London. The text for picture 22, retinopathy of prematurity, was written by Dr Clare Gilbert. Dr Clare Gilbert also updated the text in 2007.
The text and slides have been reviewed by Dr Allen Foster, Professor Simon Franken, Dr Clare Gilbert, Professor Gordon Johnson and Ms Sue Stevens.
Photographs and artwork used in this teaching set are gratefully acknowledged:
- John D C Anderson – Pictures 19a, 19b, 20a, 24a
- Christoffel Blindenmission – Pictures 8c, 10a 10b, 24b
- Allen Foster – Pictures 6b, 12c, 13d, 11b, 11c, 15d, 17b, 18a, 19c, 23a
- Simon Franken – Pictures 4d, 6a
- Clare Gilbert – Pictures 16a, 22a
- Iris Medical Instruments – Pictures 22b, 22c, 22d
- Gordon Johnson – Pictures 6d, 19a
- Volker Klauss – Pictures 21a, 21b
- Hans Limburg – Picture 12d
- Gawn McIlwaine – Picture 23b
- Murray McGavin – Pictures 4a, 4b, 5, 8a, 8b, 8d, 12a, 13a, 13b, 13c, 15a, 17a, 18b, 20, 24d
- Donald McLaren – Picture 6c
- John Sandford-Smith – Pictures 11a, 15b
- Jonathan Sladden – Picture 4c
- Erika Sutter – Picture 12b
- UNICEF – Picture 24c
- David Yorston – Pictures 11d,15c, 16b
Supported by CBM International, HelpAge International, Sight Savers International, Task Force Sight and Life.
© 1998, updated 2007. International Centre for Eye Health, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, United Kingdom